
Quick answer
A stress fracture is a small crack — sometimes more like a deep bone bruise — that develops when bone is loaded harder than it can absorb. In the foot, it’s almost always from doing too much, too soon. The classic story: a runner who recently increased mileage, pain that builds with activity and gets worse the next day. Catch it early and recovery takes 6–8 weeks. Ignore it and it becomes a real fracture.
Where they happen in the foot
The most common locations:
- Metatarsals 2 and 3 — the long bones of the second and third toes. Sometimes called a “march fracture” from the historical association with new soldiers.
- Calcaneus (heel) — runners, military recruits
- Navicular — high-impact athletes; this one is high-risk (poor blood supply, slow to heal, often missed on early X-rays)
- Fifth metatarsal — at the base; the Jones fracture zone is high-risk
Symptoms
The hallmark pattern:
- Pain that starts mild and builds with activity
- Pinpoint tenderness when you press on the affected bone
- Pain that eases with rest initially, but resumes when you start activity again
- Worse the next day after a hard workout
- Sometimes swelling over the affected area
- Often no obvious “injury” — the patient can’t recall a specific moment it started
If you suspect a stress fracture and keep pushing through the pain, eventually:
- Pain becomes constant
- The bone may complete its fracture (now a true fracture)
Why they happen
Bone is constantly remodeling — old bone is broken down, new bone is built. Normally these stay in balance. Stress fractures happen when the load exceeds the bone’s ability to repair.
The big triggers:
- Sudden increase in training — new mileage, new sport, new shoes
- Hard surfaces — concrete, asphalt
- Worn-out shoes with poor cushioning
- Foot mechanics — high arches transmit more force; flat feet can shift load
- Relative Energy Deficiency in Sport (REDs) — formerly the “female athlete triad”; the IOC and major sports-medicine bodies now use REDs because the syndrome affects all genders and involves more systems than the original triad. Insufficient energy intake relative to training load drives bone loss, hormonal disruption, and increased stress fracture risk.
- Vitamin D deficiency — increasingly recognized contributor
- Smoking — impairs bone healing
- Certain medications — long-term steroids, some other meds
What else it could be — the differential diagnosis
Stress fracture is a clinical pattern (insidious, activity-related forefoot or midfoot pain) that overlaps with several other conditions. Several of these are commonly mistaken for stress fracture, or vice versa:
- Acute (true) fracture — a discrete moment of injury you may not remember; standard fractures and stress fractures look different on imaging but can present with similar pain
- MTP capsulitis — joint-capsule inflammation that produces tenderness at the metatarsal head rather than along the shaft
- Plantar plate tear — partial or complete tear of the plantar capsule of an MTP joint, often with toe drift; tenderness is plantar to the MTP head, not on the bone shaft
- Freiberg’s disease (avascular necrosis of the metatarsal head) — osteonecrosis of a lesser metatarsal head; classically the second metatarsal in adolescent girls, but can occur in adults. Easily confused with stress fracture clinically and often on early X-rays.
- Morton’s neuroma / interdigital neuritis — burning or electric pain into adjacent toes from compressive nerve irritation between the metatarsals
- Sesamoiditis or sesamoid fracture — when pain is under the first metatarsal head specifically
- Bone bruise / contusion — bone marrow edema without a fracture line
- Tendinitis, tenosynovitis, or peroneal tendon problems — soft-tissue overuse along the dorsum or sides of the foot
- Metatarsalgia — diffuse forefoot pain from overload, fat-pad atrophy, or general mechanical issues
- Tarsal coalition, arthritis, or accessory navicular — for atypical midfoot or hindfoot pain
- Soft-tissue infection or osteomyelitis — uncommon but important when there is a wound or systemic illness
This is why a clinician’s evaluation matters — and why MRI rather than plain X-ray is often the test that resolves the picture, particularly when X-rays are normal in the first few weeks.
Diagnosis
This is one of the trickier diagnoses in foot care because plain X-rays are normal in the first 2–3 weeks. The bone hasn’t started healing visibly yet.
- Plain X-ray — first step; may show changes 2–6 weeks in (callus formation)
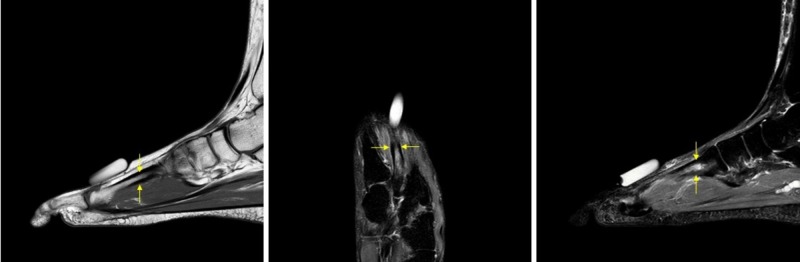
- MRI — most sensitive; can detect a stress reaction before any fracture line forms
- Bone scan — alternative when MRI isn’t accessible
- CT — sometimes used for navicular fractures
If your symptoms fit a stress fracture and X-rays are normal, don’t assume it isn’t one. The diagnosis is often made on the basis of clinical pattern + repeat imaging or MRI.
Treatment
The treatment is simple in concept, hard in practice: stop loading the bone, let it heal.
Low-risk stress fractures (most metatarsals, calcaneus)
- Activity modification — no running, jumping, or pain-producing activities for 6–8 weeks
- Cross-training — swimming, cycling, upper-body work to maintain fitness
- Stiff-soled shoe or walking boot for 2–4 weeks if the foot hurts walking
- Ice and NSAIDs sparingly (NSAIDs may slow bone healing — short courses only)
- Address the cause — nutrition, training program, shoes
High-risk stress fractures (navicular, 5th metatarsal Jones zone, sesamoid)
These need non-weight-bearing for 6–8 weeks (crutches, wheelchair) and sometimes surgical fixation, particularly in athletes who need to return to sport reliably.
Return to running
Gradual. Common protocol:
- Pain-free walking for 1–2 weeks
- Walk-jog progression
- Slow buildup of mileage (the “10% rule”)
- Total return to pre-injury training: typically 12+ weeks from initial diagnosis
When to see a clinician
- Pain that builds over days to weeks during training
- Pinpoint tenderness on a specific bone
- Pain that doesn’t resolve after 1–2 weeks of rest
- Inability to complete normal training despite reduced load
- Pain in a high-risk location (navicular, fifth metatarsal base, sesamoids)
- Athlete with signs of low energy availability or menstrual irregularities and bone pain (screen for REDs)
Prevention
- Build mileage gradually — the “10% rule” is a starting point, not a guarantee
- Replace shoes every 300–500 miles
- Surface variety — alternate hard surfaces with softer ones
- Cross-train instead of always running
- Adequate nutrition — calcium, vitamin D, sufficient calories for training load
- Address signs of low energy availability (REDs) — including menstrual irregularities, persistent fatigue, or unintended weight loss
- Don’t run through pain — early action saves weeks of recovery
Bottom line
Stress fractures are an overuse injury, not an accident. The pain builds gradually, is focal to one bone, worsens with activity, and improves with rest. A normal X-ray in the first 2 to 3 weeks does not rule one out — MRI is the test of choice when symptoms fit the pattern. Treatment is conceptually simple (stop loading the bone) but takes 6 to 8 weeks for low-risk locations and longer for high-risk sites (navicular, Jones zone, sesamoids). If you’re a runner with new pinpoint foot pain that’s been building for a week or two, see a clinician before it completes into a true fracture.
Frequently asked questions
How do I know if I have a stress fracture in my foot?
The hallmark pattern: pain that builds during activity, eases with rest, and is worse the next day after a hard workout. Press along each bone of the forefoot — pinpoint tenderness on a specific bone, especially the 2nd or 3rd metatarsal, points to a stress fracture. Pain that came on without a single moment of injury and that has been getting worse over weeks is the classic story. A normal X-ray does not rule it out; MRI is the test of choice in the first 2 to 3 weeks.
How long does a foot stress fracture take to heal?
Low-risk sites (tibia, metatarsal shafts, calcaneus) typically heal in 6 to 8 weeks of activity modification. High-risk sites (femoral neck, navicular, 5th metatarsal base) often require 8 to 12+ weeks, sometimes with non-weight-bearing protocols or surgical fixation. Full return to running usually takes 12 or more weeks from diagnosis. Trying to push through accelerates the timeline in the wrong direction — a missed stress fracture can complete and become a true fracture that needs surgery.
Can you walk on a stress fracture in your foot?
Often yes, painfully. That's part of why these are missed — people walk on them for weeks. But continuing to walk normally lets the crack progress. The right approach is activity modification: stiff-soled shoe or walking boot for 2 to 4 weeks if the foot hurts walking, no running or jumping for 6 to 8 weeks. High-risk locations (navicular, Jones zone, sesamoids) require non-weight-bearing on crutches, not just no running.
What does a stress fracture in the foot feel like?
Like a deep, aching, pinpoint pain on one specific bone, usually in the forefoot. It builds with activity, fades with rest, and is sharper the morning after a hard workout. Unlike soft-tissue overuse pain (which spreads across an area), stress fracture pain is focal — you can usually point to it with one finger. Mild swelling on top of the foot over the painful spot is common.
What causes stress fractures in the foot?
Doing too much, too soon. The bone can't repair as fast as the load is breaking it down. Common triggers: a sudden increase in running mileage, a new sport, new shoes (especially minimalist), hard surfaces (concrete, asphalt), worn-out shoes with no cushioning, foot mechanics (high arches or flat feet), Relative Energy Deficiency in Sport (REDs — formerly the female athlete triad), vitamin D deficiency, smoking, and long-term steroid use.
Are stress fractures and Jones fractures the same thing?
Not exactly. A Jones fracture is a specific fracture at the base of the fifth metatarsal in Zone 2, a 'watershed' area with poor blood supply. It can happen acutely (a sudden twist) or as a stress fracture from chronic loading. Jones fractures have a notoriously high non-union rate — ranging from 11% to over 50% in some conservative management studies — compared to other metatarsal fractures. Many require surgical fixation, especially in athletes who need to return to sport reliably.
Sources
Last updated: May 3, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 3, 2026