Quick answer
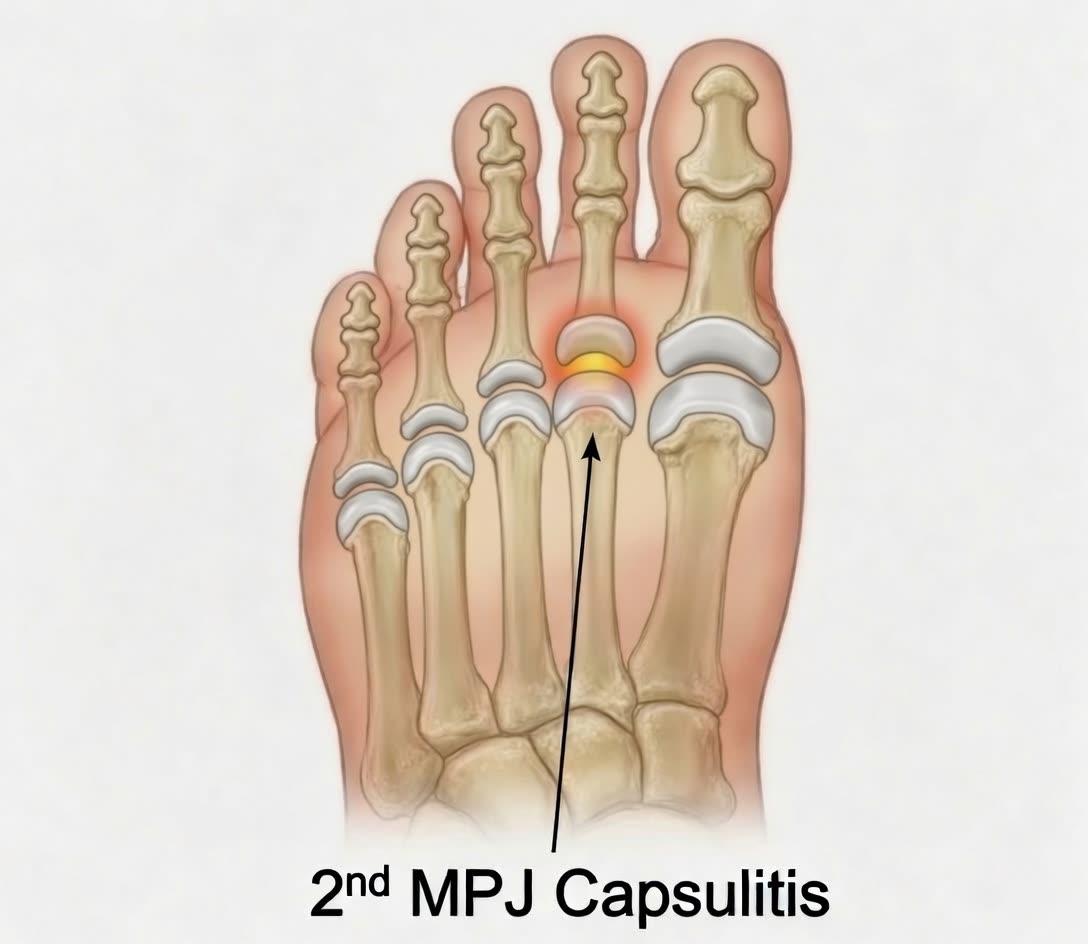
MTP capsulitis is inflammation of the joint capsule — the ligamentous wrapper — around a metatarsophalangeal (MTP) joint at the base of a lesser toe. The second MTP joint is by far the most common location. It’s often the early stage of a more serious problem: a plantar plate tear. Caught early, capsulitis usually responds well to conservative measures.
How to recognize it
- Pain at the ball of the foot under the second toe (less commonly third or fourth)
- Swelling at the base of the toe
- A feeling of walking on a marble or wadded sock
- Pain with barefoot walking on hard surfaces
- Worse in tight or narrow shoes
- Pain with push-off — going up on the toes, climbing stairs
- Subtle drift of the toe — sideways or upward — in later stages
In contrast to a fully torn plantar plate, the toe in pure capsulitis hasn’t visibly drifted yet. The structures are inflamed but still anatomically intact.
A surface lesion sitting directly under the same MTP joint — most commonly porokeratosis plantaris discreta (PPD) — can produce point-tender forefoot pain that mimics capsulitis on history alone. A careful look at the bottom of the foot is part of the diagnosis, since PPD has a discrete central plug and is treated with in-clinic debridement, not joint-directed care.
Why this happens
Capsulitis develops when the second MTP joint is chronically overloaded. The joint capsule and surrounding plantar plate take more stress than they can absorb, and inflammation builds up over weeks to months.
Common contributors:
- Long second toe — naturally bears more load
- Bunion deformity — the big toe deviates and stops carrying its share, shifting load to the second
- High heels — push body weight forward onto the metatarsal heads
- Narrow toe boxes — cram and squeeze the forefoot
- High arches — fewer points of contact with the ground, more pressure on the metatarsal heads
- High-impact activities — running, jumping, dancing
- Increasing age — soft tissues lose elasticity
The capsulitis–plantar plate spectrum
It’s easiest to think of these as a single continuum:
- Capsulitis — pain, inflammation, no structural failure. Reversible.
- Pre-dislocation syndrome — capsule weakens; subtle drift starts. Still potentially reversible.
- Plantar plate tear — partial or complete structural failure. Surgical repair usually needed for full correction.
- Dislocation — toe sits over or beside another. Surgical correction needed.
The earlier you catch this, the simpler the treatment.
Diagnosis
- Physical exam — tenderness on the bottom of the affected MTP joint, swelling, Lachman test of the toe (gentle vertical stress on the toe to check stability)
- Inspection — looking for early drift compared to the other foot
- X-rays — rule out stress fractures, arthritis; may show subtle MTP changes
- Ultrasound — useful for distinguishing pure capsulitis from an early plantar plate tear
- MRI — for cases that aren’t clear on exam or ultrasound
Treatment
Conservative care (the standard, often successful)
The goal is to offload the painful joint and let it calm down.
- Stiff-soled shoes — limit painful motion at the joint
- Wide toe boxes — eliminate crowding
- Metatarsal pad — placed just behind the metatarsal heads to lift load off the painful joint. Often dramatically helpful within days.
- Toe taping (buddy taping the second toe to the third) — adds stability
- Custom orthotics with metatarsal padding for chronic cases
- NSAIDs short-term for inflammation
- Activity modification — temporary reduction in running, dancing, time in heels
- Avoid steroid injections at the MTP joint — they can weaken the plantar plate and accelerate progression to a tear
- Address the cause — bunion treatment, heel height, training load
Most cases of true capsulitis (without structural tear) respond to these measures within 6–12 weeks.
When more is needed
- Walking boot or stiff post-op shoe for 2–4 weeks for severe inflammation
- Repeat imaging if pain persists despite good conservative care — looking for a tear
Surgery
Surgery is generally reserved for cases that have progressed beyond pure capsulitis to a structural plantar plate tear. For details on those procedures, see the plantar plate tear guide.
Bottom line
MTP capsulitis is the early, treatable stage of a problem that — if ignored — turns into a plantar plate tear and a drifting toe. The most useful single intervention is a metatarsal pad placed correctly, combined with stiffer-soled shoes and reducing the load on the joint. Catching it before structural damage develops is the difference between a few weeks of conservative care and potential surgery years later.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026