Quick answer
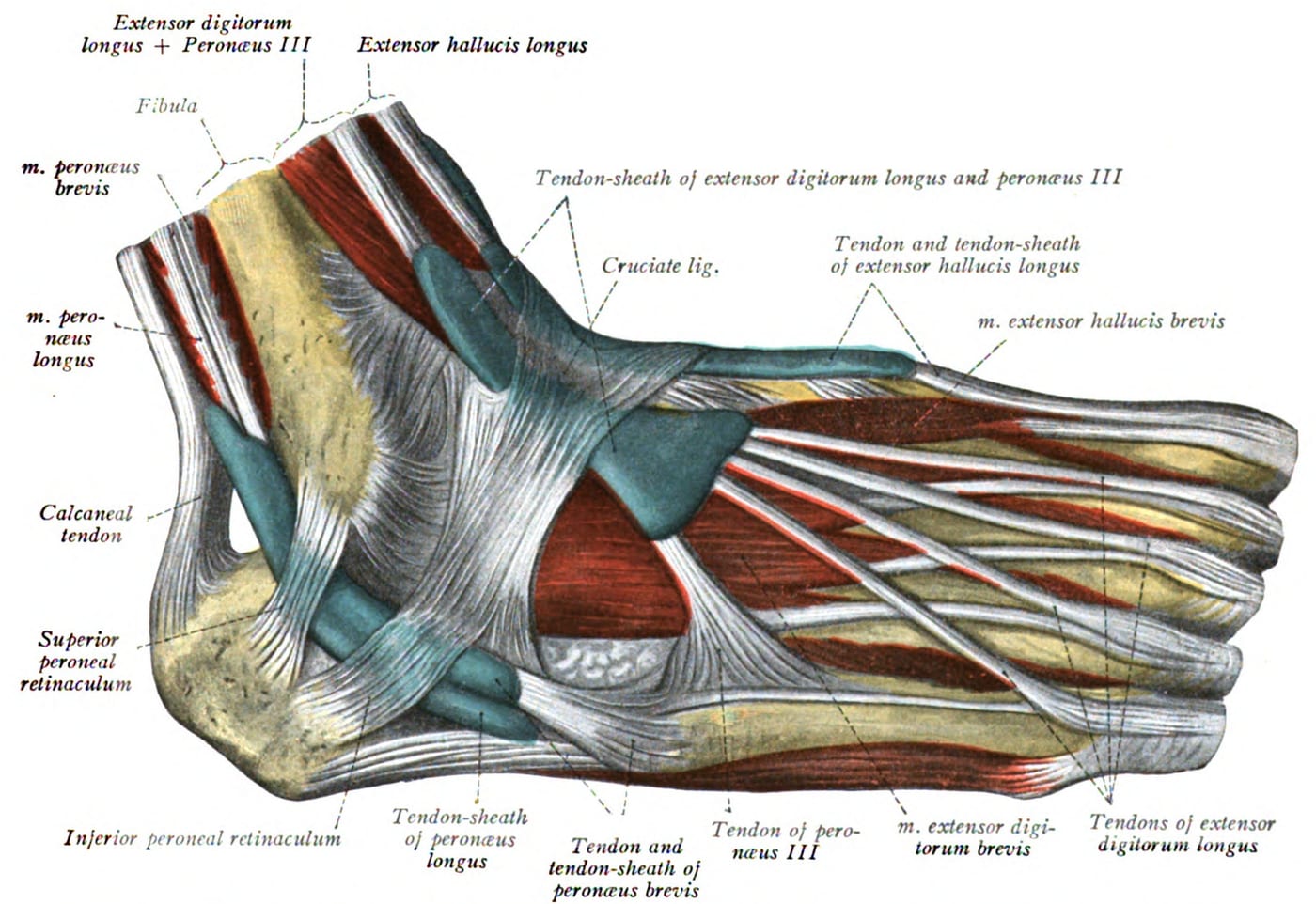
The extensor tendons run across the top (dorsum) of the foot and lift the foot and toes upward. The main ones are:
- Tibialis anterior — the largest, lifts the foot
- Extensor hallucis longus — lifts the big toe
- Extensor digitorum longus — lifts the lesser toes
- Peroneus tertius (when present)
Extensor tendinitis is inflammation of any of these — most commonly the tibialis anterior or extensor hallucis longus. It produces aching pain on top of the foot that’s worse with activity and pressure.
Why it happens
- Tight shoe lacing — by far the most common cause. The tendons get compressed against the metal eyelets and bone underneath
- Sudden increase in running, especially hill running and downhill running (eccentric loading on the extensors)
- Walking on uneven ground for extended periods (hiking, walking tours)
- High arch foot — concentrates dorsal forces on the tendons
- Bone spurs on the dorsum — can rub against the tendons (often coexists with midfoot arthritis)
- Sudden footwear changes — switching to a stiff or new shoe
The tendons themselves don’t usually have a structural problem; they’re irritated by external pressure or load.
How to recognize it
- Pain on top of the foot along the line of the tendons
- Tenderness when pressing along the tendon path
- Pain worse with active foot lift or toe extension against resistance
- Pain worse with shoes, especially tightly-laced shoes
- Sometimes a creaking or crepitus when the tendon is moved
- Mild swelling along the tendon
- Often relieved by removing shoes and resting the foot
A simple test: have the patient lift their foot upward against resistance. If the dorsal pain reproduces, extensor tendinitis is likely.
Diagnosis
Almost always a clinical diagnosis based on history and exam. Workup includes:
- History — recent activity changes, shoe history
- Exam — pain along the tendons, pain with resisted dorsiflexion or toe extension
- X-rays — to rule out a stress fracture or dorsal bone spurs (a common contributor)
- MRI or ultrasound — only if symptoms persist despite appropriate conservative care, or if the diagnosis is unclear
Treatment
The vast majority of cases resolve with simple measures:
First-line care
- Loosen shoe lacing — the single most effective step. Skip eyelets directly over the painful spot, or switch to a shoe with a different lacing pattern
- Rest from aggravating activity for 1–2 weeks
- Ice after activity
- NSAIDs for inflammation
- Padding under the laces — small foam or felt pads to redistribute pressure
- Switch shoes if a particular pair is the culprit
- Reduce running mileage temporarily, then build back gradually
For runners, a typical pattern: rest 5–7 days, then return to easy running while gradually rebuilding mileage. Avoid hills until pain-free.
If it doesn’t resolve
- Physical therapy — eccentric calf and shin strengthening; gait analysis
- Custom orthotics — if foot mechanics (high arch, overpronation) are contributing
- Cortisone injection — selectively, around (not into) the tendon. Generally reserved because of tendon rupture risk near injections
- Imaging to rule out other causes (stress fracture, dorsal bone spurs, ganglion cyst)
Surgery
Rarely needed. Reserved for:
- Cases with structural causes — bone spurs causing chronic friction, or specific tenosynovitis from a mass effect
- Surgical decompression involves removing the offending bone or tissue
Bottom line
Extensor tendinitis is one of the easiest foot problems to fix — most cases resolve with looser lacing, rest, and ice. Persistent cases warrant evaluation for underlying contributors (high arch, dorsal spurs, training errors). Surgery is rarely needed. If you’re a runner with new top-of-foot pain, check your laces and shoe wear pattern before anything else.
Last updated: April 27, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 27, 2026