Quick answer
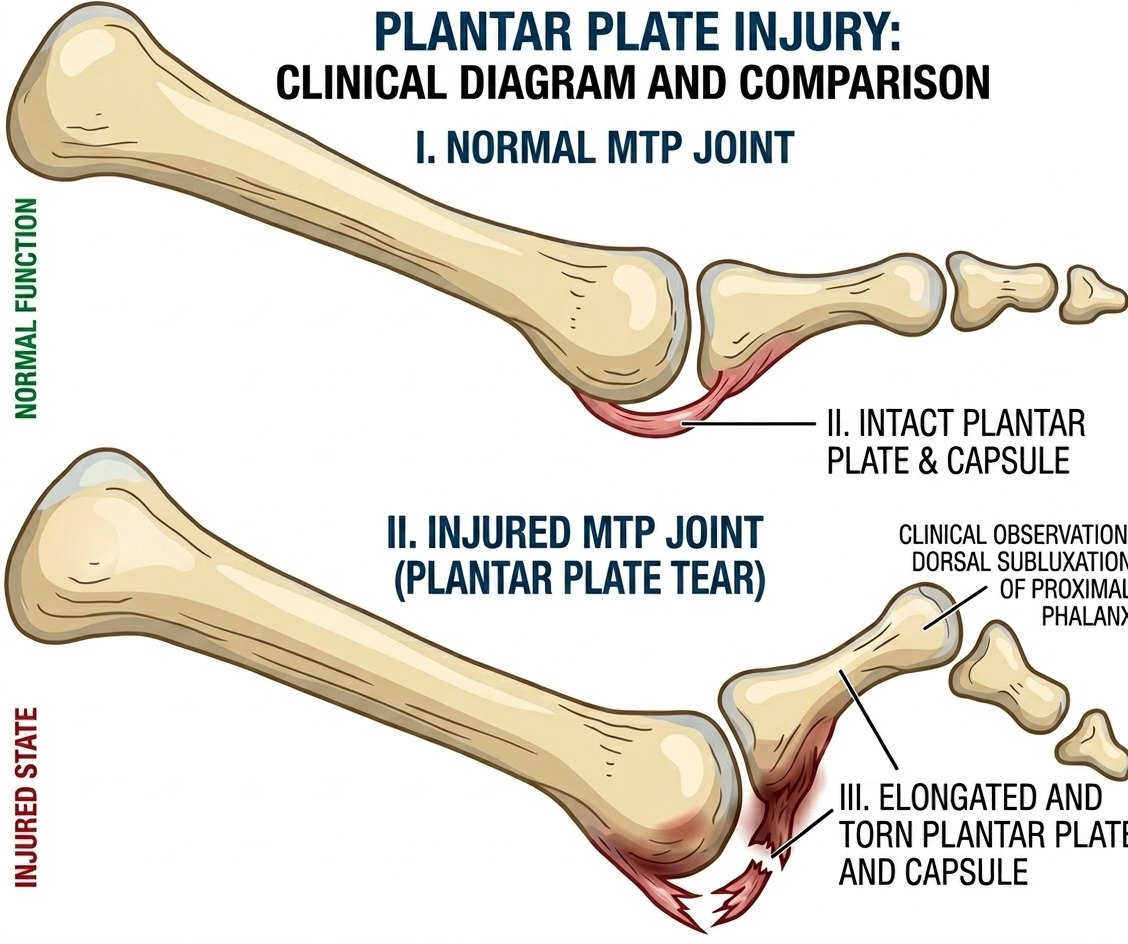
The plantar plate is a thick fibrocartilage ligament on the bottom of each metatarsophalangeal (MTP) joint. It anchors the toe and prevents it from drifting upward or sideways. When this plate tears — usually at the second MTP joint — the toe loses its anchor and gradually drifts out of position. The result: forefoot pain, a “crossover toe,” or a “floating toe” that no longer touches the ground.
Anatomy in plain terms
Each lesser toe (toes 2–5) has an MTP joint at its base. The joint is held together by:
- The joint capsule above
- Collateral ligaments on each side
- The plantar plate below — the strongest of these stabilizers
The plantar plate functions like a ligamentous floor of the joint. It absorbs load during push-off and prevents the toe from extending too far upward.
When the plate fails — either gradually from chronic stress or acutely from a forced extension — the toe drifts. The second toe is most often affected because it bears the most load (especially when the first toe is shifted by a bunion).
How to recognize it
- Pain at the ball of the foot under the affected toe (most often the second)
- Swelling at the base of the toe
- A toe that’s drifting — sideways toward the big toe, or upward off the ground
- “Crossover toe” — second toe rides over or under the big toe in advanced cases
- “Floating toe” — the affected toe doesn’t touch the ground when standing
- Feeling like walking on a marble under the ball of the foot
- Pain with push-off — going up on the toes, walking barefoot
The progression is usually:
- Capsulitis (inflammation, pain, no deformity)
- Pre-dislocation (subtle drift, increasing pain)
- Plantar plate tear (toe drifts visibly)
- Dislocation (toe sits over or to the side of an adjacent toe)
Why it happens
Common contributors:
- Long second toe — bears excess load
- Bunion deformity — the big toe stops carrying its share, second toe takes over
- High-heeled or pointy shoes — cram the forefoot and chronically extend the toes
- High-impact activities — running, dancing, jumping
- Inflammatory arthritis (rheumatoid, psoriatic) — weakens the plate
- Steroid injections at the MTP — may accelerate plate failure
- Increasing age — connective tissue changes
Most cases are gradual, the result of years of overload rather than a single injury.
Diagnosis
- Physical exam — tenderness directly under the MTP joint, swelling, and the Lachman test of the toe (or “drawer test”): a clinician grasps the toe and shifts it up and down. Excessive vertical motion compared to the other side suggests a tear.
- Inspection — the affected toe is usually visibly drifting
- X-rays — rule out other causes (stress fracture, arthritis); the toe deformity may be visible
- Ultrasound — can show the tear, increasingly used as a first-line confirmatory test
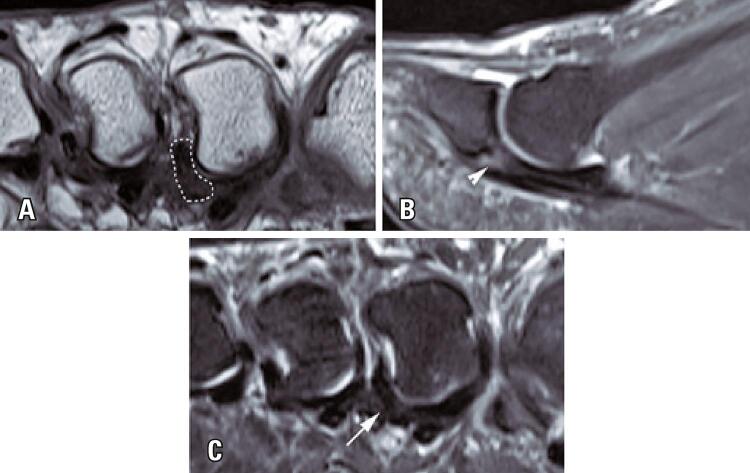
- MRI — gold standard for soft tissue detail; clearly shows the plantar plate
Treatment
Conservative care (first-line for early-stage tears)
The goal: stabilize the toe, redistribute load, and reduce inflammation.
- Stiff-soled shoes — limit motion at the painful joint
- Wide toe box — relieve crowding
- Metatarsal pad — placed just behind the metatarsal heads to offload the painful joint
- Toe taping — pulling the affected toe downward and toward neutral can hold it in better alignment during healing
- Custom orthotics — for chronic cases, with metatarsal padding built in
- Activity modification — reduce running, jumping, time in heels
- NSAIDs for inflammation
- Avoid corticosteroid injections at the MTP joint — they can accelerate plate failure
- Physical therapy — intrinsic foot strengthening
Conservative care can stabilize symptoms and prevent progression but generally doesn’t reverse a structural tear. Realistic goal: pain relief and stability, not anatomic repair.
Surgery
For tears that fail conservative care, especially when the toe is significantly drifted:
- Direct plantar plate repair — sutures reattach the torn plate, often combined with shortening osteotomies of the metatarsal (Weil osteotomy) to take tension off the repair
- Tendon transfer — borrowing a tendon to substitute for the failed plate (older technique, less common now)
- Toe shortening procedures — to address a long second toe contributing to the problem
- Recovery typically 3–6 months
- Outcomes are best when the toe deformity is mild-to-moderate; severe drift is harder to fully correct
Bottom line
A plantar plate tear is the structural endpoint of long-standing forefoot overload — usually under the second MTP joint. Catching it early (at the capsulitis stage) and addressing the load with stiff shoes, met pads, and orthotics can prevent the toe from drifting. Once the toe has visibly shifted, conservative care may stabilize it but surgery is usually needed for full correction.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026