
Quick answer
An accessory navicular is an extra small bone or piece of cartilage located on the inner side of the midfoot, just behind the arch — next to the regular navicular bone. About 4–14% of people have one, most of whom never know it. When it becomes painful, it typically presents as arch pain in adolescents or active adults.
How to recognize it
When symptomatic:
- Pain on the inside of the arch, just in front of the medial ankle
- A visible bony bump at the inner arch
- Tenderness when pressing on the bump
- Pain with activity, especially running, jumping, or dancing
- Worse in tight shoes or shoes that rub against the prominence
- Sometimes pain after a twisting injury that strained the connection
- Can mimic posterior tibial tendon dysfunction — and the two often coexist
The bump is usually visible to the naked eye, especially when standing — it sits about a thumb’s width forward and slightly downward from the inner ankle bone.
The three types
Accessory naviculars are classified by anatomy:
- Type I — a small sesamoid bone within the posterior tibial tendon. Usually asymptomatic. About 30% of accessory naviculars.
- Type II — connected to the navicular by a fibrocartilaginous bridge (synchondrosis). The most commonly symptomatic type. About 50–60% of cases.
- Type III — fused to the navicular as a bony prominence (sometimes called “cornuate navicular”). Symptoms when the prominence rubs on shoes.
The type matters because it influences treatment — Type II responds best to surgery if needed; Type III is more about footwear modification.

Why this becomes painful
Most accessory naviculars are silent. Pain typically develops because:
- Adolescent growth spurt — the connection between accessory and main navicular is stressed
- Trauma — an inversion injury sprains or breaks the synchondrosis
- Increase in activity — new sport or training intensity
- Posterior tibial tendon strain — the tendon attaches to or near the accessory bone, transmitting force
- Footwear pressure — narrow or stiff shoes rub the prominence
- Flat feet — the posterior tibial tendon works harder, stressing the attachment
Because the posterior tibial tendon plays such a central role in arch support, an unstable accessory navicular can contribute to flat feet — and vice versa.
Diagnosis
- Physical exam — tenderness over the prominence, sometimes pain with resisted foot inversion
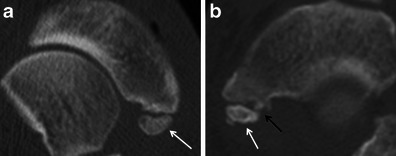
- X-rays — show the accessory bone and its type
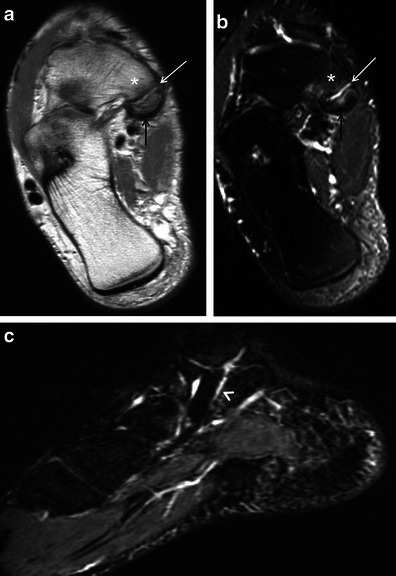
- MRI — looks for inflammation at the synchondrosis (a Type II that’s “hot”) and posterior tibial tendon involvement
- Bone scan — occasionally used to confirm the accessory is the source of pain
Treatment
Conservative care (first-line for most)
- Activity modification — reduce activities that aggravate pain
- Wider shoes with soft padding over the prominence — eliminate direct pressure
- Custom orthotics with arch support and a medial post — unloads the posterior tibial tendon
- NSAIDs for inflammation
- Walking boot for 4–6 weeks for severe pain or after acute injury — often allows the synchondrosis to settle
- Physical therapy — posterior tibial tendon strengthening, calf stretching
- Cortisone injection in selected cases
A significant majority of symptomatic accessory naviculars settle with conservative care, especially after a flare related to growth or new activity.
Surgery
For pain that doesn’t respond to 3–6 months of dedicated conservative care:
- Kidner procedure — the classic surgery: removes the accessory bone and reattaches the posterior tibial tendon to the main navicular. Generally well-tolerated.
- Modified Kidner — variations on the above
- Synchondrosis fusion — joins the accessory to the main navicular as a single bone
- Recovery typically 6–12 weeks; non-weight-bearing initially, then progressive
- Outcomes are generally good in well-selected patients
If posterior tibial tendon dysfunction has developed alongside the accessory navicular, surgery may need to address both.
Bottom line
Most accessory naviculars are anatomic curiosities that never cause trouble. When they do, it’s usually in adolescence or after a change in activity. Footwear modification, orthotics, and a course of relative rest resolve most symptomatic cases. Surgery (the Kidner procedure) is well-established for cases that don’t respond — but it’s reserved for genuinely persistent pain after a real trial of conservative care.
Frequently asked questions
What is an accessory navicular bone?
An accessory navicular is an extra small bone (or piece of cartilage) on the inside of the midfoot, adjacent to the normal navicular bone, where the posterior tibial tendon inserts. It's present in roughly 10–14% of people — a normal anatomical variant rather than a disease. Most people with one never know it exists. A small subset develops pain from the extra bone being irritated or from the attached tendon being stressed.
What are the three types of accessory navicular?
Geist's classification recognizes three types. Type 1 is a small (2–3 mm) round bone embedded within the posterior tibial tendon, usually painless. Type 2 is a larger (10–12 mm) bone connected to the main navicular by a synchondrosis (a cartilage joint) — the most common painful type. Type 3 is a true bony enlargement of the navicular itself ('cornuate navicular'), forming a prominent bump on the inside of the foot but usually not painful.
Does an accessory navicular cause flat feet?
Not directly. The accessory bone changes where the posterior tibial tendon inserts, which can affect how the arch is supported. People with a symptomatic accessory navicular often also have flat feet, and the combination can accelerate posterior tibial tendon dysfunction. But a small accessory navicular alone in someone with a normal arch usually doesn't cause flatfoot to develop.
Do I need surgery for accessory navicular?
Most cases respond to conservative care — supportive shoes, custom orthotics that offload the inner midfoot, activity modification, and short courses of NSAIDs. Surgical excision (the Kidner procedure) is reserved for pain that doesn't respond after several months of conservative care. The procedure removes the accessory bone and reattaches the posterior tibial tendon. Recovery is roughly 6–8 weeks in a boot followed by gradual return to activity.
How do I know if my arch pain is from an accessory navicular?
The classic story is pain on the inner side of the midfoot, where you can usually feel a bony prominence about an inch in front of the inner ankle bone. Pressing directly on that bump reproduces the pain. The pain often worsens with running, hiking, or activities that load the arch. A plain X-ray confirms the diagnosis — the accessory bone is usually clearly visible.
Sources
Last updated: May 3, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 3, 2026