Quick answer
A Jones fracture is a specific kind of fifth metatarsal fracture — at the junction between the base and the shaft of the bone, on the outside of the foot. The location matters: this part of the bone has notoriously poor blood supply, so these fractures heal slowly and often need surgery, especially in athletes.
The three zones
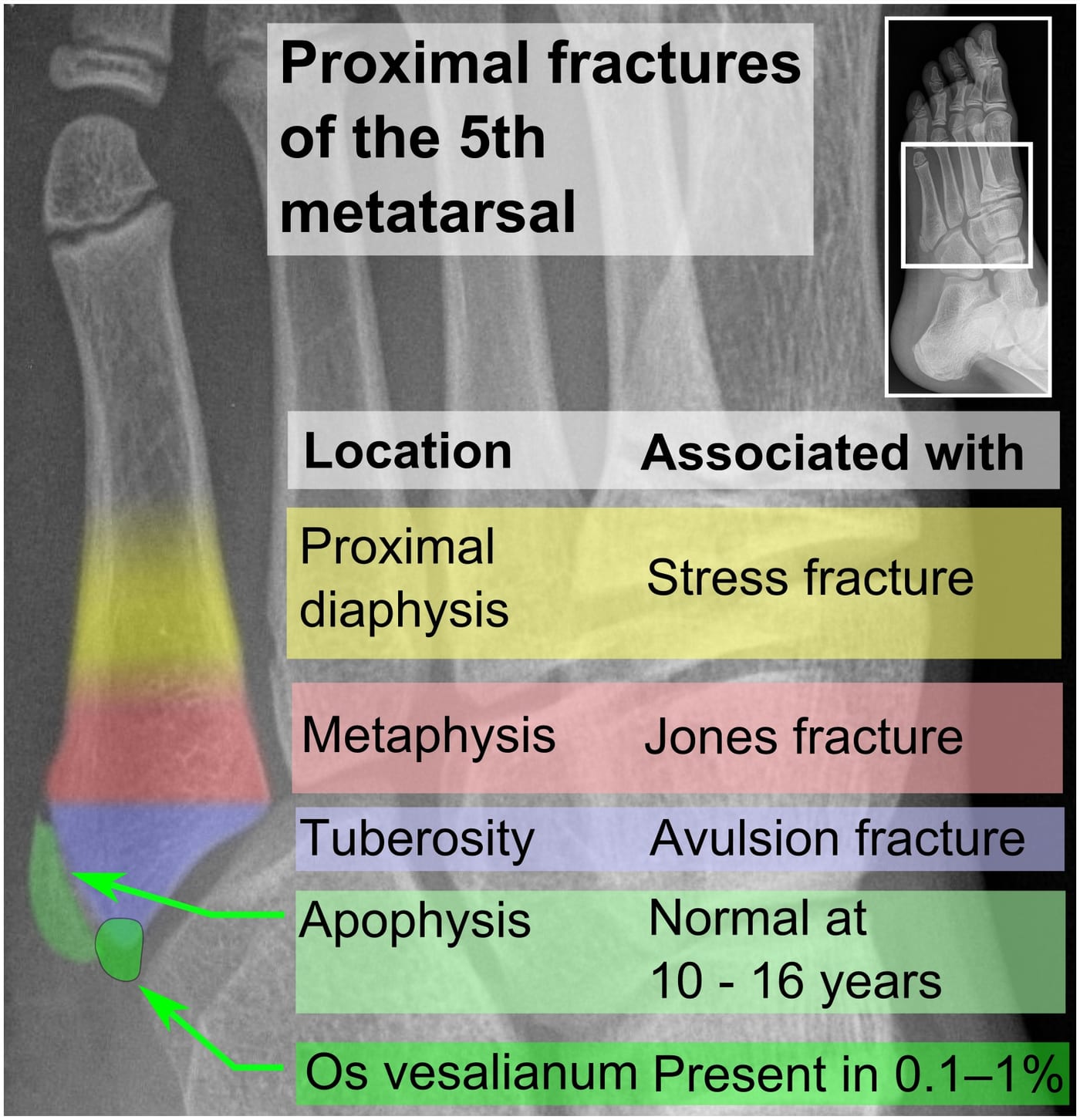
The fifth metatarsal base is divided into three zones, and the zone determines treatment:
- Zone 1 — Avulsion fracture (the tip): a chip pulled off by the peroneus brevis tendon. Heals reliably with a walking boot or stiff shoe.
- Zone 2 — True Jones fracture (the metaphyseal-diaphyseal junction): the watershed area with poor blood supply. Slow to heal, prone to non-union.
- Zone 3 — Proximal diaphyseal stress fracture: a fatigue fracture of the shaft, common in athletes with high arches. Also slow to heal.
The distinction matters — they all look similar on X-ray to the untrained eye, but they’re managed very differently. Calling every fifth metatarsal fracture a “Jones fracture” is one of the most common mistakes in foot injuries.


How to recognize it
- Sudden pain on the outside of the foot after an injury
- Often a forceful inward roll of the ankle (inversion)
- Bruising and swelling along the lateral foot
- Inability to bear weight — or only able to walk with a limp
- Tenderness when pressing on the base of the fifth metatarsal
- For stress fractures, pain develops gradually over weeks of training, worse with activity
Why these heal so slowly
The blood supply to the proximal fifth metatarsal comes from a few small arteries that converge in a watershed area — the same region where Jones fractures occur. When the bone breaks, those vessels are often disrupted, leaving the fracture line with marginal blood flow.
Without good blood supply, bone healing stalls. This is why:
- Healing takes 8–20 weeks even with proper treatment
- Non-union (fracture never heals) occurs in 15–30% of conservatively treated cases
- Refracture is common after return to sport
- Athletes are often offered surgery upfront to get back faster and more reliably
Diagnosis
- Physical exam — point tenderness over the proximal fifth metatarsal
- X-rays — three views (AP, lateral, oblique) of the foot
- MRI — used when stress fractures are suspected but X-rays are normal
- CT scan — sometimes used to assess for non-union or pre-operative planning
A clinician will look carefully at where the fracture line is — millimeters can change the treatment plan.
Treatment
Zone 1 (avulsion fractures)
Generally heal well with conservative care:
- Walking boot or stiff-soled shoe for 3–6 weeks
- Weight-bearing as tolerated in most cases
- Return to sport typically 6–8 weeks
Zone 2 (true Jones) and Zone 3 (proximal diaphyseal stress fractures)
This is where management gets nuanced:
Conservative approach:
- Non-weight-bearing cast or boot for 6–8 weeks, then progressive weight bearing
- Total healing time 3–4 months
- Higher rates of non-union and refracture
Surgical approach (often preferred for athletes):
- Intramedullary screw fixation — a screw is inserted down the shaft of the bone
- Faster, more reliable healing
- Return to sport typically 8–12 weeks
- Lower refracture rate
- Becoming the standard for competitive athletes and active adults
The choice between conservative and surgical care depends on activity level, the specific zone, and the patient’s goals.
Adjuncts
- Bone stimulators — external low-intensity pulsed ultrasound or pulsed electromagnetic field devices, sometimes used to accelerate healing in slow-healing fractures or established non-unions. A practical note on insurance: in many US clinics the realistic timeline for getting a bone stimulator approved is around 90 days from the date of the first X-ray of the injury — the device generally has to be requested for “delayed union” rather than from day one, and the documentation requirements vary substantially by insurer. If you want one, expect a wait and ask your surgeon’s office to start the prior-authorization paperwork early.
- Vitamin D and calcium optimization — particularly important in stress fractures
- Address the cause — for stress fractures, evaluate training load, foot mechanics (high arches), and bone health
Bottom line
Not all fifth metatarsal fractures are the same — the zone matters enormously, and even a few millimeters of difference can change the treatment from “boot for six weeks” to “surgery and three months out.” Avulsion fractures generally heal reliably; true Jones fractures and proximal stress fractures are stubborn, with non-union rates of 15–30% in conservatively treated cases. Any acute lateral foot injury with bruising, swelling, or inability to bear weight needs same-day in-person evaluation and X-rays — this is not a fracture pattern to manage from a website. Treatment decisions (boot vs. cast vs. surgery, weight-bearing vs. non-weight-bearing) need to come from a clinician who has seen your X-rays and examined your foot.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026