Quick answer
Osteomyelitis is an infection of bone. In the foot, it most commonly occurs as a complication of diabetic foot ulcers — bacteria from the ulcer spread downward through soft tissue and eventually into the underlying bone. It can also follow foot trauma, surgery, or spreading soft tissue infection. Osteomyelitis is notoriously difficult to diagnose without imaging and difficult to eradicate without prolonged antibiotic therapy or surgical debridement. It’s a leading reason for foot and lower leg amputation.
Why the foot
The foot is the most common site for osteomyelitis in adults in the developed world, primarily because of diabetic foot disease. Several factors combine to make diabetic feet especially vulnerable:
- Neuropathy — loss of protective sensation means wounds go unnoticed
- Peripheral arterial disease — impaired blood flow reduces immune response
- Hyperglycemia — impairs white blood cell function
- Foot deformities and pressure points — from Charcot foot, hammertoes, bunions
- Skin breakdown — ulcers create a direct route for bacteria
Once a foot ulcer forms and becomes infected, bacteria can spread through soft tissue to reach the bone below — sometimes within days.
How to recognize it
The challenge: osteomyelitis in the diabetic foot is often clinically silent in early stages. The neuropathy that caused the ulcer also masks the deep, throbbing bone pain that would otherwise be a warning sign.
Clinical clues:
- A non-healing foot ulcer despite good wound care (lasting more than 2–4 weeks)
- Probing to bone — a sterile cotton swab inserted into the wound hits bone. This finding is ~85% specific for osteomyelitis.
- “Sausage toe” — diffuse swelling of a toe due to infection in the toe bones
- Visible or palpable bone in the wound
- Persistent bone pain and swelling, particularly in the midfoot or toe
- Normal-appearing ulcer overlying a recently fractured or deformed bone
- Failure of cellulitis or soft tissue infection to improve with antibiotics
Systemic signs (more variable than in acute osteomyelitis elsewhere):
- Fever (often absent or low-grade in diabetic patients)
- Elevated white blood cells, CRP, ESR (ESR >70 mm/hr is suggestive)
How bacteria get to the bone
Three main routes:
- Contiguous spread — the most common in the foot. Bacteria from a wound, ulcer, or soft tissue infection spread directly into adjacent bone.
- Hematogenous (bloodstream) — less common in the foot. Bacteria in the bloodstream seed the bone, more typical in children (vertebral osteomyelitis in adults).
- Direct inoculation — after trauma, surgery, or a puncture wound that directly contaminates bone.
In diabetic foot disease, contiguous spread from an ulcer is the dominant mechanism.
Bacteria involved
Unlike most other infections, diabetic foot osteomyelitis is often polymicrobial (multiple organisms):
- Staphylococcus aureus — most common single organism
- MRSA — increasingly common, particularly in patients with prior antibiotic exposure or healthcare contact
- Streptococcal species
- Gram-negative rods (Pseudomonas, Proteus, Enterobacter) — especially in chronic wounds
- Anaerobes — in deep, poorly perfused, necrotic wounds
Identifying the specific organisms matters because antibiotic choice depends on culture results.
Diagnosis
Getting the diagnosis right is critical — osteomyelitis requires a fundamentally different treatment approach than soft tissue infection alone.
Imaging
- X-rays — first test. Look for bone erosion, cortical destruction, periosteal reaction. X-rays lag 2–4 weeks behind disease — often normal in early osteomyelitis.
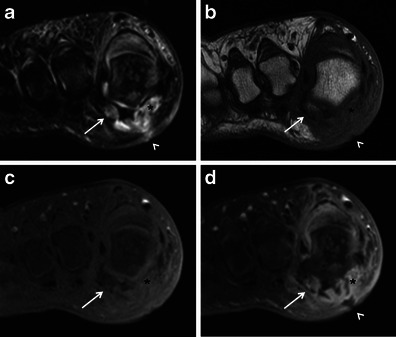
- MRI — the gold standard for soft tissue and early bone involvement. Shows bone marrow edema, cortical destruction, and soft tissue extension. Highly sensitive and specific. Most useful when X-rays are ambiguous.
- Bone scan (technetium) — sensitive but not specific; often positive in any active bone process
- CT scan — shows cortical destruction well; useful for surgical planning
- WBC-labeled scan or PET — for equivocal cases
Bone biopsy / culture
The definitive diagnosis: a specimen of infected bone sent for culture and pathology. Tells you exactly what organism you’re treating and whether viable bone is left.
Methods:
- Percutaneous CT-guided biopsy — in an office or radiology suite
- Intraoperative biopsy — during surgical debridement
Swab cultures of wounds or ulcers are unreliable for osteomyelitis — they sample surface organisms, not the ones in the bone.
Lab markers
- ESR >70 mm/hr — one of the most useful screening findings
- CRP, WBC — elevated in many but not all cases
- Blood cultures — positive in a minority; important when bacteremia is possible

Treatment
Osteomyelitis of the foot is serious and typically requires a multi-pronged approach.
Antibiotics — the cornerstone
- Oral antibiotics are surprisingly effective for diabetic foot osteomyelitis, despite the severity of the diagnosis. Multiple trials support prolonged oral therapy (with appropriate agents) as equivalent to IV therapy for many patients.
- IV antibiotics — for MRSA, severe infections, or patients unable to absorb oral medications
- Duration — typically 6–12 weeks for medically managed osteomyelitis
- Antibiotic choice based on bone culture results whenever possible
Antibiotic choice depends on the organism identified on culture and susceptibility testing — typically agents active against staphylococci (including MRSA when present) and, for diabetic foot cases, often broader-spectrum coverage. Your infectious-disease specialist or surgeon selects the regimen and route.
Surgery
Often necessary — and sometimes the faster, more reliable path to cure:
- Debridement — surgical removal of infected, necrotic bone. Leaves viable bleeding bone behind.
- Minor amputation — resection of an infected toe or metatarsal head. Can be definitive treatment when confined to a limited area.
- Goals of surgery: remove the source of ongoing infection, allow wound closure, preserve as much functional foot as possible
Osteomyelitis is often a medical-surgical problem — antibiotics control the systemic infection, surgery removes the infected tissue.
Wound care
Treating the wound that caused the problem:
- Offloading — total contact cast or removable cast walker to get pressure off the ulcer
- Debridement of devitalized wound tissue
- Advanced wound dressings or negative pressure wound therapy
- Vascular assessment — if blood flow is impaired, revascularization may be needed for the wound to heal at all
Vascular surgery
Poor circulation dramatically impairs healing. Patients with peripheral arterial disease often need vascular surgery consultation and possibly revascularization (angioplasty or bypass) before osteomyelitis can be eradicated.
When amputation is considered
Amputation is the outcome no one wants, but sometimes it’s the right treatment:
- Extensive bone involvement that can’t be adequately debrided
- Failed multiple rounds of antibiotics
- Persistent infection despite surgery
- Severe arterial insufficiency without revascularization options
- Sepsis from the foot threatening life
The goal is always to amputate as little as possible — a toe amputation is very different from a below-knee amputation. Early, aggressive management of diabetic foot osteomyelitis is aimed at avoiding the higher amputations.
Prevention
In people with diabetes:
- Daily foot inspection — looking for wounds that “shouldn’t be there”
- Prompt treatment of foot wounds — small ulcers caught early are easily treated; the same ulcer infected for 3 months is a much harder problem
- Properly fitting footwear — therapeutic shoes and custom orthotics to eliminate pressure points
- Aggressive glycemic control — impairs wound healing and immune function when poorly controlled
- Annual foot exams with a clinician
- Treat athlete’s foot promptly — a common gateway for foot infection
- Regular podiatry visits for patients with neuropathy or prior ulcers
When to seek care — and how urgently
Emergency department / 911 if any of the following:
- Fever, chills, or feeling unwell with a foot wound
- Red streaks spreading up the foot or leg
- Severe pain, especially in a foot that is normally numb
- Blackening, gray, or rapidly darkening tissue
- Confusion, rapid heart rate, dizziness, or low blood pressure with a foot infection (possible sepsis)
- A wound visibly enlarging in 24 hours
Same-day clinic visit for:
- A foot wound that has not healed in 4 weeks (or 2 weeks in a person with diabetes)
- A wound where bone is visible or you can probe to bone with a sterile swab
- Any foot infection that has not improved within 48–72 hours of starting oral antibiotics
- Unexplained deep foot pain in someone with diabetes or a prior ulcer
- New “sausage toe” (diffuse swelling of one toe) — concerning for osteomyelitis of the toe bones
Do not assume a non-healing wound is “just slow.” In diabetes, a non-healing wound is a wound that needs imaging.
Bottom line
Osteomyelitis of the foot is one of the most serious, and most preventable, complications of diabetic foot disease. The key is catching it early: a non-healing ulcer, a wound that probes to bone, or any foot infection that isn’t improving with antibiotics should prompt imaging (MRI) and clinical evaluation. Treatment requires prolonged antibiotics, often surgery, meticulous wound care, and vascular assessment. Early, aggressive management — not delayed, minimal treatment — is what keeps major amputations off the table.
Sources
Last updated: May 3, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 3, 2026