

What it is
An ingrown toenail occurs when the corner or side of a toenail curls down and grows into the soft skin next to it. The big toe is by far the most common location — it bears the most weight and pressure during walking.
In medical terms it’s called onychocryptosis (from Greek: onycho = nail, crypto = hidden). The “ingrown” part is slightly misleading — the nail isn’t actually growing inward; rather, the skin and the nail are colliding, and the nail edge breaks the skin’s protective barrier.
The condition typically progresses through three stages:
- Inflammation — the side of the toe is red, swollen, and tender. No drainage yet.
- Infection — bacteria enter through the broken skin. Drainage, pus, increased pain, possible fever.
- Granulation tissue — chronic cases develop a fleshy overgrowth of tissue alongside the nail.
Symptoms
Early signs:
- Tenderness along the side of the toenail, especially the big toe
- Redness and mild swelling at the nail margin
- Discomfort when wearing closed shoes or putting pressure on the toe
Later stages:
- Throbbing pain, particularly when standing or walking
- Pus, drainage, or bleeding from the nail margin
- A small bump of red, sometimes shiny tissue at the side of the nail (granulation)
- Fever or red streaks moving up the foot — signs of spreading infection
What causes it
The most common triggers:
- Cutting nails too short or rounding the corners — when the nail grows back, the corner can catch on the skin instead of growing past it
- Tight shoes that compress the toes
- Sports trauma — repetitive impact (running, soccer, ballet) or a single stub
- Naturally curved nail shape — some people are simply prone to it
- Improper nail clipping technique — using rounded nail scissors or “digging out” the corners
- Sweaty feet that soften the nail and surrounding skin
- Genetic predisposition
Certain conditions also increase risk: fungal nail infections, abnormal toe positioning (hammertoe, hallux valgus), and conditions affecting circulation or sensation.
Watch out — not every persistent “ingrown toenail” is actually an ingrown. If a painful nail border keeps returning despite repeat clipping and conservative care, especially in a younger person, the underlying problem may be a subungual exostosis — a small bone growth pushing up under the nail. A lateral X-ray makes the diagnosis.
Treatment options
Treatment depends on the stage. Mild cases can often be managed at home; established infections or recurrent cases need professional care.
At-home care for early/mild cases (no infection)
- Soak the foot in warm, soapy water for 15–20 minutes, two to three times daily
- Gently lift the nail edge with a small piece of cotton or dental floss tucked under it after soaking, to encourage the nail to grow above the skin
- Apply antibiotic ointment and a clean bandage
- Wear roomy, open shoes — sandals if possible — to avoid pressure
- Take over-the-counter pain relievers (acetaminophen or ibuprofen) as needed
Do not “dig out” the nail or attempt bathroom surgery. This usually makes things worse and increases infection risk.
If symptoms don’t improve within a few days, or if signs of infection develop, see a clinician.
Professional treatment
For infections, recurrent cases, or unrelenting pain, a podiatrist can perform a quick in-office procedure:
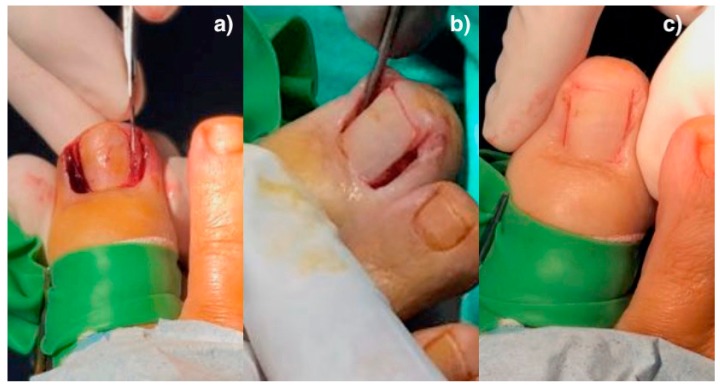
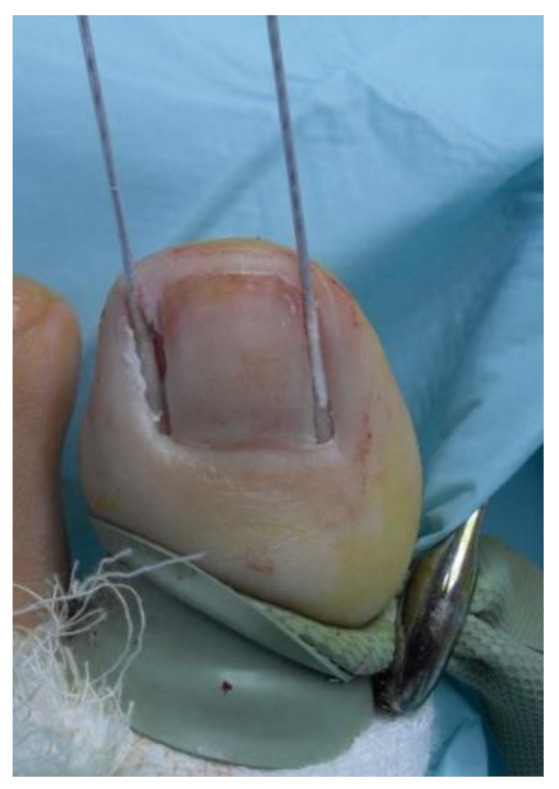
- Partial nail avulsion — under local anesthetic, the offending edge of the nail is removed. The toe heals over 2–4 weeks. The nail grows back in most cases.
- Partial nail avulsion with matrixectomy — same as above, but the underlying nail-growing tissue (matrix) at the affected edge is destroyed (chemically with phenol, or surgically). This permanently prevents that strip of nail from regrowing — typically used for recurrent ingrown nails. Success rate >90%.
- Antibiotics — for established infections, often given alongside the procedure
- Drainage of any abscess
The procedure itself takes 10–20 minutes, healing involves daily soaks and dressing changes, and most people return to normal shoes within a couple of weeks.
When to see a clinician
Make an appointment if:
- Pain is severe or limiting your ability to walk
- Drainage, pus, or significant redness is present
- The toe is hot to the touch or you have a fever
- This is a recurring problem
- The skin alongside the nail has developed a fleshy bump (granulation tissue)
- You have diabetes, peripheral artery disease, or any condition affecting circulation or sensation — even mild ingrown nails can become serious in this group, and you should not attempt at-home treatment
Prevention
The single most effective change: how you trim your nails.
- Cut straight across, not curved
- Don’t trim too short — leave a small amount of nail beyond the nail bed
- Use proper toenail clippers, not scissors or fingernail clippers
- Trim after a bath or shower when nails are softer
- Avoid tight shoes — particularly narrow toe boxes
- Wear properly-fitted athletic shoes for sports
- Keep feet dry to prevent the skin from softening
- If you’re prone to ingrown nails, consider seeing a podiatrist for routine nail care
A note for people with diabetes
Ingrown toenails in people with diabetes are not the same problem they are for everyone else. Reduced sensation can mask the early stages, reduced circulation impairs healing, and the consequences of an infected toe can include hospitalization or worse. Do not attempt at-home treatment — see a clinician at the first sign of any toenail problem.
Frequently asked questions
How do you get rid of an ingrown toenail at home?
Mild cases often resolve with: warm soaks for 15–20 minutes 3–4 times daily, gently lifting the nail edge with a small piece of cotton, applying antibiotic ointment, and wearing roomy open shoes. Don't dig out the corner — that usually makes it worse and risks infection. If symptoms don't improve in a few days, see a clinician.
When should I see a doctor for an ingrown toenail?
See a clinician if there's pus, spreading redness, fever, severe pain, fleshy overgrowth at the side of the nail, or if you have diabetes. A persistent infection of the nail fold itself is called paronychia and may need antibiotic treatment in addition to drainage. Recurrent ingrown nails in the same toe usually need a small in-office procedure to permanently fix.
Will an ingrown toenail heal on its own?
Mild ingrown nails sometimes resolve with home care alone (soaks, lifting the edge, roomier shoes). More established cases — especially with infection or fleshy overgrowth — usually need professional treatment. Ignoring an infected ingrown nail can lead to deeper infection.
How is an ingrown toenail removed?
A podiatrist numbs the toe with a local anesthetic injection, then removes the offending edge of the nail (partial nail avulsion). For recurrent cases, the underlying nail-growing tissue (matrix) is also destroyed — chemically with phenol or surgically — so that strip of nail doesn't grow back. The procedure takes 10–20 minutes.
How long does it take an ingrown toenail to heal after removal?
After a partial nail avulsion, expect 2–4 weeks of daily soaks and dressing changes. Most people return to normal shoes within 2 weeks. If the nail matrix was destroyed (matricectomy), success is over 90% — that strip of nail doesn't regrow.
Can ingrown toenails be prevented?
The single biggest prevention: cut nails straight across, not curved. Don't trim too short, use proper toenail clippers, and avoid narrow toe boxes. People prone to ingrown nails often benefit from regular professional nail care, especially if they have neuropathy or trouble reaching their feet.
Sources
- Muriel-Sánchez JM, Becerro-de-Bengoa-Vallejo R, Montaño-Jiménez P, Coheña-Jiménez M. The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. J Clin Med. 2020;9(3):845. (CC BY 4.0) ↗
- Muriel-Sánchez JM, Coheña-Jiménez M, Montaño-Jiménez P. Effect of Phenol Application Time in the Treatment of Onychocryptosis: A Randomized Double-Blind Clinical Trial. Int J Environ Res Public Health. 2021. (CC BY 4.0) ↗
Last updated: May 1, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 1, 2026