What it is
A bunion is what you see when the big toe joint has gradually drifted out of alignment over years. The first metatarsal bone rotates and shifts toward the midline of the body while the big toe angles toward the second toe — and the metatarsophalangeal (MTP) joint itself becomes the prominent, often painful bump along the inner border of the forefoot.
The bump itself is bone — not a growth. The joint is actually being pushed out of alignment over time. The medical term is hallux valgus (“hallux” = big toe, “valgus” = leaning outward).


AP foot X-rays compared — left: normal alignment. Right: hallux valgus, with the big toe drifting laterally and the first metatarsal angling medially. Surgeons measure the hallux valgus angle (HVA) and intermetatarsal angle (IMA) on these views to grade severity. Images: Wagner & Wagner, 2024 (CC BY 4.0).
Symptoms
Common signs people report:
- A visible bump on the inside of the foot at the big toe joint
- Pain or soreness around the joint, especially when walking
- Swelling, redness, or warmth at the bump
- Restricted movement of the big toe
- Calluses where the first and second toes rub — and sometimes a deeper, more focal porokeratosis plantaris discreta (PPD) under a lesser metatarsal head when the bunion shifts weight-bearing pressure laterally
- Difficulty finding shoes that fit comfortably
Symptoms often appear gradually and may worsen with prolonged standing or activity.
What causes it
Bunions develop from a combination of factors. Genetics is the strongest predictor — if a parent had bunions, the foot structure that predisposes you to one is often inherited. Other contributors:
- Foot shape and biomechanics (low arches, loose ligaments)
- Years of wearing narrow, pointed, or high-heeled shoes
- Inflammatory conditions like rheumatoid arthritis
- Previous foot injury
Shoes alone don’t cause bunions, but tight footwear can accelerate progression in someone already predisposed.
Treatment options
Treatment depends on how much the bunion interferes with daily life. Most people are managed without surgery.
Conservative (non-surgical)
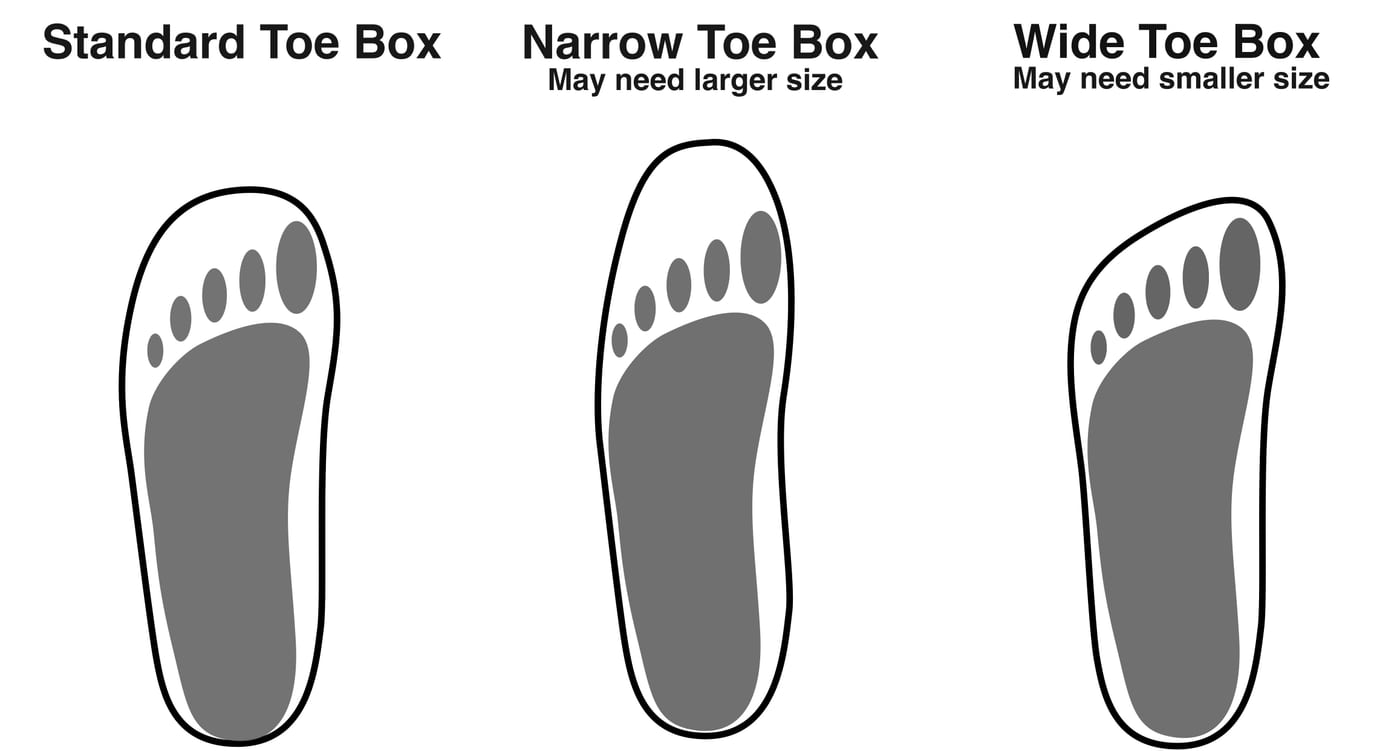
- Wider shoes with a roomy toe box — often the single most impactful change
- Bunion pads or spacers to reduce friction and pressure
- Custom orthotics to redistribute weight across the foot
- NSAIDs (ibuprofen, naproxen) for pain and inflammation, used short-term
- Ice after activity for sore, swollen joints
- Toe exercises to maintain joint mobility
These approaches don’t reverse the deformity, but they can keep symptoms manageable for years.
Surgical
When pain limits walking or daily activity despite conservative care, bunion surgery (a bunionectomy) may be considered. There are over 100 described procedures for correcting a bunion — that variety exists because no single operation is right for every foot. The right operation depends on the severity of the deformity, the angles measured on weight-bearing X-rays, the condition of the joint, your age, your activity level, and your goals.
The most common procedures used today fall into a few broad categories:
- Austin (chevron) osteotomy — a V-shaped cut near the head of the first metatarsal that lets the bone be shifted into better alignment, then held with a screw. One of the most widely used procedures for mild-to-moderate bunions with a healthy joint. Typically done through a small incision; outpatient.
- Lapidus procedure (first tarsometatarsal joint fusion) — for moderate-to-severe bunions, especially when there is hypermobility at the base of the first metatarsal. The operation fuses the joint between the first metatarsal and the medial cuneiform, addressing the deformity at its root. Generally requires a longer period of protected weight-bearing.
- First MTP joint fusion (arthrodesis) — usually reserved for severe deformity with significant arthritis at the big toe joint (often overlapping with hallux rigidus). The big toe joint is permanently fused in a functional position. You give up motion at that joint — including whatever range of motion you had before surgery. In return, you get a reliably pain-free joint that holds up well over decades. Most patients walk and even run normally afterward; high heels are no longer comfortable.
- Minimally invasive bunion surgery (MIS) — a relatively new family of techniques that use small incisions and specialized burrs to make the bone cuts and fix them with screws percutaneously. Reduced soft-tissue trauma, smaller scars, and often faster early recovery. Outcomes in experienced hands are comparable to open techniques for appropriately selected patients, but the results are very surgeon-dependent and the procedure requires specific training.
- Exostectomy alone (“bump-only” bone shave) — removes the prominent bump without realigning the bone. Almost always insufficient as a stand-alone procedure for a true bunion — because the underlying alignment problem isn’t corrected, the bump tends to come back. Reserved for select cases where alignment is already acceptable and only the prominence is symptomatic.
Other procedures (proximal osteotomies, scarf osteotomies, Akin osteotomy of the proximal phalanx as an adjunct, soft-tissue rebalancing) round out the list. Most bunion surgeries combine elements — for example, an Austin osteotomy with a soft-tissue rebalance and an Akin to address residual toe deviation.
Why the right choice depends on a specialist visit, not a website
Bunion surgery is highly individualized. Picking the right operation requires:
- Weight-bearing X-rays of both feet to measure the specific angles (intermetatarsal angle, hallux valgus angle, distal metatarsal articular angle, sesamoid position) and assess joint health
- An in-person exam to check joint flexibility, hypermobility at the first ray, range of motion, calluses, and adjacent toe deformities
- A frank conversation about goals — return to running, fitting into specific shoes, pain-free walking, cosmetic improvement, willingness to accept a longer recovery for a more durable result, willingness to accept loss of motion in exchange for a reliably pain-free fusion, etc.
- Your medical history — diabetes, peripheral arterial disease, smoking, prior foot surgery, and inflammatory arthritis all change risk profiles and which procedure makes sense
Like any surgery, bunion correction carries real risks — recurrence (the bunion comes back, more common with under-correction or non-compliance with post-op restrictions), under- or over-correction (including hallux varus — the toe drifts the other way), stiffness, transfer metatarsalgia, persistent pain, neurovascular injury, infection, non-union (after fusion or osteotomy), hardware problems, wound healing problems, and anesthetic risks. Recovery typically takes 6–12 weeks for return to walking shoes, with full healing and final shape over 6–12 months.
This page is general educational information. Decisions about whether and how to operate on a bunion need to be made in person with a board-certified foot and ankle surgeon (orthopedic or podiatric) — ideally one who performs bunion surgery regularly — after reviewing your X-rays, examining your foot, and having an unhurried conversation about which of the many available procedures fits your specific deformity, anatomy, and goals.
When to see a clinician
Book an appointment if you notice:
- Persistent pain that limits walking or activity
- Inability to find shoes that fit
- Visible deformity that’s getting worse
- Numbness, tingling, or burning at the joint
- Redness and warmth that could suggest infection or inflammation
Early evaluation gives you the most options and helps slow progression.
Living with it
Many people manage bunions for decades without surgery. Practical tips:
- Get fitted for shoes in the afternoon, when feet are slightly larger
- Look for shoes with a wide toe box, soft upper, and low heel
- Replace worn shoes — collapsed support accelerates symptoms
- If you exercise, choose lower-impact activities (swimming, cycling) on flare-up days
Frequently asked questions
Can a bunion be reversed without surgery?
No — once the bone has shifted, conservative treatment can't realign it. But supportive shoes, orthotics, toe spacers, and pads can dramatically reduce pain and slow progression. Many people manage bunions for decades without surgery.
Do bunions get worse over time?
Bunions tend to progress gradually, especially with continued narrow-shoe wear or in people with the inherited foot structure that predisposes them. The rate varies — some bunions stay stable for years; others progress steadily. Pain doesn't always track with severity.
Are bunions caused by shoes?
Not directly — genetics is the strongest predictor. If a parent had bunions, you've inherited the foot mechanics that make them likely. Tight, pointed, or high-heeled shoes don't cause bunions on their own, but they accelerate progression in people who are already predisposed.
What is the best shoe for bunions?
A shoe with a wide, deep toe box, soft uppers (no seams pressing on the bump), low heel, and good arch support. Avoid pointed-toe shoes, narrow athletic shoes, and high heels. Some people benefit from extra-depth shoes that accommodate orthotics.
How painful is bunion surgery recovery?
Most patients describe moderate pain for the first few days, well-controlled with prescription pain medication. Recovery to walking shoes typically takes 6–12 weeks; full healing and final shape develops over 6–12 months. Pain usually isn't the limiting factor — it's the strict weight-bearing restrictions and time off your feet.
Can you walk after bunion surgery?
Yes, in a special post-op shoe or boot — but with strict weight-bearing limits (heel-only walking, or a knee scooter) for the first 2–6 weeks depending on the procedure. Returning to normal shoes typically happens around 6–12 weeks. Returning to running takes 4–6 months.
Sources
Last updated: May 1, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 1, 2026