What it is
Hammertoe, mallet toe, and claw toe are three closely related toe deformities — they share most causes, most non-surgical treatments, and many of the surgical procedures used to correct them. The difference is which joint is bent, and how many.
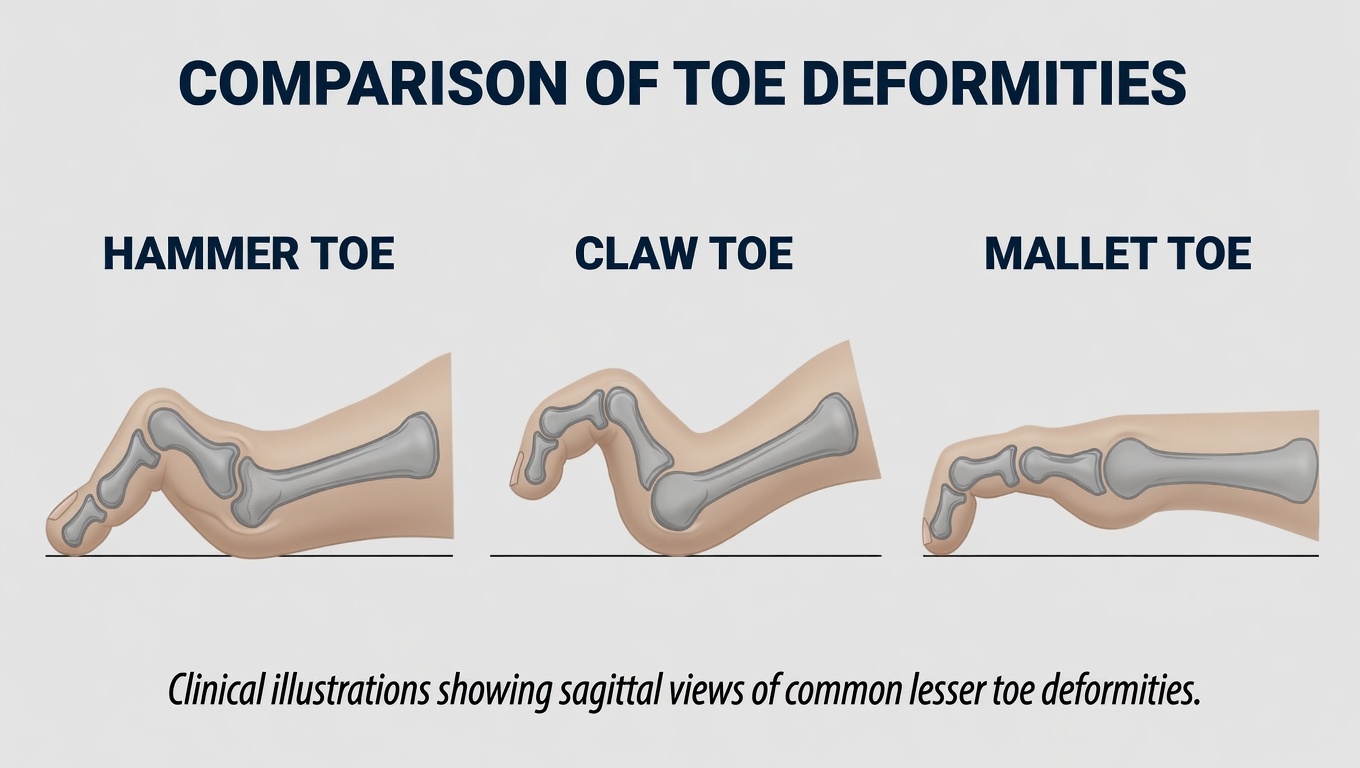
Quick comparison
| Deformity | MTP joint (base) | PIP joint (middle) | DIP joint (tip) | Most typical look |
|---|---|---|---|---|
| Mallet toe | Normal | Normal | Bent down | Tip points straight down; rest of toe straight |
| Hammertoe | Normal | Bent up (kinked) | Normal | Middle of toe forms an upside-down “V” |
| Claw toe | Bent up | Bent down | Bent down | Whole toe curls under like a claw |
All three commonly affect the second, third, or fourth toes. The big toe is rarely involved (when the big toe is affected, it’s usually a different problem like hallux rigidus). Early on, these deformities are flexible — you can manually straighten the toe. Over time, they become rigid, locked into the bent position. Flexible vs. rigid matters more than the specific deformity name when deciding treatment.
Symptoms
- Visible bend in one or more toes
- Pain at the top of the bent joint, where it rubs against the shoe
- Calluses or corns on the prominent areas — the top of the bent joint, the tip of the toe, or between toes
- Difficulty finding shoes that don’t aggravate the toe
- Pain at the ball of the foot (the bent toe causes weight to shift, overloading the metatarsal heads). Chronic pressure under a metatarsal head from a hammertoe can also produce a small, deep keratotic lesion called porokeratosis plantaris discreta (PPD) — sharply painful for its size and often mistaken for a callus or wart.
- In severe cases, blisters, ulcers, or wounds — a particular concern for people with diabetes
What causes it
These deformities develop from imbalance between the muscles, tendons, and ligaments that control the toe. When the small intrinsic foot muscles weaken or the longer extrinsic tendons over-pull, the toe gradually deforms.
Common contributors:
- Tight or pointed shoes — especially years of wearing shoes that crowd the toes
- High heels — push toes forward into the front of the shoe
- Bunions — the big toe pushing on the second toe is a classic cause
- Foot mechanics — flat feet, high arches, and neuromuscular conditions
- Arthritis — particularly rheumatoid arthritis affecting the toes
- Trauma — a previous toe injury can predispose
- Genetics — foot shape is largely inherited
Treatment options
Treatment depends on whether the toe is flexible or rigid.
Conservative care (works best for flexible deformities)
- Roomy footwear — wide toe boxes, soft uppers, low heels. The single most impactful change.
- Orthotics or metatarsal pads — redistribute pressure off the ball of the foot
- Toe pads, sleeves, or splints — cushion and reposition the toe
- Stretching exercises — manually straightening the toe and stretching the tendons several times daily
- Strengthening exercises — picking up small objects with the toes, towel scrunches
- Padding for calluses and corns — safe over-the-counter pads (avoid medicated “corn removers” if you have diabetes or poor circulation)
These don’t reverse the deformity but can prevent progression and significantly reduce symptoms.
Surgical correction (when conservative care fails or the deformity is rigid)
Several surgical approaches exist, often combined for a single toe:
- Tendon transfer — for flexible deformities, repositions tendons to rebalance the toe
- Joint resection (arthroplasty) — removes a small piece of bone at the bent joint to allow it to straighten
- Joint fusion (arthrodesis) — permanently fuses the bent joint in a straight position; very reliable for rigid deformities
- Tendon release / lengthening — cuts or lengthens tight tendons to allow the toe to straighten
- MTP joint procedures — for claw toes or severe hammertoes where the base joint is also extended; may include capsule release, tendon transfer, or osteotomy
- Calf or Achilles lengthening — sometimes added when calf tightness is contributing
Most procedures are outpatient. Recovery typically involves a stiff post-op shoe for 4–6 weeks, with pin or screw fixation, and full healing over 3–6 months.
Risks of surgical correction
Surgical correction of a hammertoe, mallet toe, or claw toe is generally a successful procedure — but it is not minor, and it carries real risks that should be discussed in detail with your foot and ankle surgeon before deciding. Realistic published complication rates for these procedures range from roughly 10–30% depending on the technique used, how rigid the deformity is, the number of toes operated on, and patient health factors. Specific risks include:
- Recurrence of the deformity — the most common complication; rates rise with rigid deformities, multi-toe surgery, and patients with underlying neuromuscular causes (claw toe in particular)
- Stiffness of the operated toe — the joint may end up straighter but more rigid; some patients trade a bent toe for a stiff one
- “Floating toe” — the operated toe no longer touches the ground, losing function in push-off and standing balance
- Overcorrection producing the opposite deformity (hyperextended or upturned toe)
- Infection — superficial wound infection is common; deep infection or osteomyelitis is rare but serious
- Neurovascular injury — the small nerves supplying the toe can be damaged, causing persistent numbness, hypersensitivity, or chronic pain. Vascular injury is rare but can rarely cause partial or complete loss of the toe (toe necrosis)
- Pin-related problems when temporary K-wires are used — pin migration, breakage, infection at the pin site, or pin tract scarring
- Hardware problems when screws or implants are used — irritation, prominence under skin, breakage, need for removal
- Non-union of a fusion — the bones fail to grow together
- Persistent or new pain at the operated toe or the metatarsal head, even after technically successful surgery
- Transfer metatarsalgia — pain shifts to the ball of the foot under the metatarsal head of the operated toe, sometimes requiring orthotics or further surgery
- Wound healing problems, especially in patients with diabetes, peripheral arterial disease, or who smoke
- Cosmetic dissatisfaction — the toe looks different from before but not “normal”
- Need for revision surgery — to address recurrence, hardware problems, or persistent symptoms
- Anesthetic risks common to any surgery
- In claw toe surgery specifically: because claw toe is usually a manifestation of diabetic neuropathy, Charcot-Marie-Tooth disease, or another neuromuscular disorder, the underlying nerve disease continues to drive the deformity — surgery does not cure that, and recurrence is more likely than for an isolated hammertoe
These risks rise in patients with diabetes (especially with neuropathy or vascular disease), smokers, those with rheumatoid or other inflammatory arthritis, and when multiple toes are operated on at the same time.
This page is general educational information and is not a substitute for an in-person evaluation. Anyone considering surgery for hammertoe, mallet toe, or claw toe should have an unhurried in-person consultation with a board-certified foot and ankle surgeon (orthopedic or podiatric). Review your X-rays, the specific procedure proposed, expected gain, recovery timeline, and the full list of risks before deciding.
When to see a clinician
Make an appointment if you notice:
- A toe that’s becoming progressively bent
- Pain that limits your shoe choice or activity
- Calluses or corns that keep coming back despite footwear changes
- A toe that’s locked in position and won’t straighten
- Any wound, blister, or persistent redness on a deformed toe — particularly important if you have diabetes
Living with it
Practical tips:
- Get fitted for shoes in the afternoon when feet are slightly larger
- Look for shoes with a wide, deep toe box and a soft, flexible upper
- Replace shoes that have developed a “memory” of your toe shape
- Use silicone toe sleeves or gel pads to cushion bent joints
- Stretch the affected toe daily — flexibility maintained is flexibility kept
- For people with diabetes, inspect feet daily; deformed toes are high-risk for ulceration
Frequently asked questions
Can hammertoes be fixed without surgery?
Flexible hammertoes (where you can manually straighten the toe) often respond well to wider shoes, toe pads, splints, and stretching exercises. Rigid hammertoes — where the toe is locked in the bent position — generally cannot be straightened without surgery, though conservative care still reduces pain. The earlier you address it, the more likely it stays flexible.
What causes hammertoes?
Hammertoes develop from imbalance between the muscles, tendons, and ligaments that control the toe. Common contributors include narrow or pointed shoes worn for years, bunions (which push the second toe), foot mechanics like flat feet or high arches, arthritis, and genetics. It's rarely a single cause — usually a combination over time.
Are hammertoe correctors and splints effective?
Splints and toe straighteners can relieve pain and slow progression in flexible hammertoes — especially when worn at night. They don't permanently 'fix' the deformity, and they don't work on rigid hammertoes. They're best thought of as symptom management, not correction.
Do hammertoes get worse over time?
Most do, gradually. A flexible hammertoe usually progresses to a rigid one over years if the underlying causes (tight shoes, biomechanical issues) aren't addressed. Pain often increases as calluses form on the bent joint and the toe rubs more in shoes.
What is the recovery time for hammertoe surgery?
Most patients are in a post-op shoe for 4–6 weeks and back in normal shoes by 6–8 weeks. Full recovery — including swelling resolution and final shape — takes 3–4 months. Pin or wire stabilization (if used) is typically removed in clinic at 4–6 weeks, often without anesthesia.
Will my hammertoe come back after surgery?
Recurrence is uncommon for isolated hammertoe corrections in healthy patients (under 10% in most series). Recurrence is more likely when there's an underlying neuromuscular cause (like diabetic neuropathy or Charcot-Marie-Tooth), with continued narrow-shoe wear, or after partial correction where the underlying mechanics weren't fully addressed.
Last updated: May 1, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 1, 2026