
What is athlete’s foot (tinea pedis)?
Athlete’s foot — known medically as tinea pedis — is a fungal skin infection of the feet caused by dermatophytes, the same group of fungi responsible for ringworm and jock itch. The name literally translates to “fungal infection of the foot” (“tinea” = fungal infection, “pedis” = foot).
The fungi thrive in warm, moist environments. Sweaty shoes are an ideal incubator. Communal damp surfaces — locker room floors, pool decks, shared showers — are common places to pick it up. Once on the skin, the fungus feeds on keratin, the protein in the outer skin layer.
It comes in four common patterns:
- Interdigital (most common) — between the toes, usually the 4th and 5th. Itchy, peeling, sometimes cracked or weeping skin.
- Moccasin — chronic dry, scaly, thickened skin on the soles and sides of the feet, in the pattern a moccasin would cover.
- Vesicular — sudden outbreak of fluid-filled blisters, often on the arch.
- Ulcerative — open sores, often with bacterial co-infection. Less common, more serious.

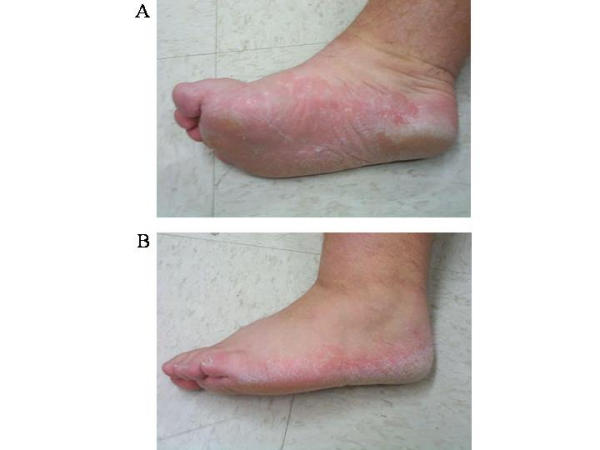

Clinical images: Al Hasan M, Fitzgerald SM, Saoudian M, Krishnaswamy G. Clin Mol Allergy. 2004;2:5. Open Access via PMC — PMC419368.
Athlete’s foot between the toes (interdigital — the most common pattern)
The space between the 4th and 5th toes is the classic site. Sweat sits there, the skin stays damp, and the fungus has the perfect environment. What you’ll see:
- Itchy, peeling skin that often gets worse after taking off shoes
- White, soft, soggy-looking skin (maceration) that may peel away in sheets
- Cracks (fissures) that can sting, bleed, or weep clear fluid
- A slightly musty smell
- Sometimes the rash spreads onto the side of the foot
This pattern is contagious through damp surfaces and easy to spread to your own shoes. Treating it without also treating the shoes (antifungal powder daily) is the most common reason it comes back within weeks.
How it looks on darker skin tones
Dermatology textbooks have historically pictured athlete’s foot on lighter skin, where erythema (redness) is the obvious sign. On darker skin tones, erythema is often less visible and may instead present as purple, violaceous, gray, or brown discoloration. The peeling, scaling, itching, and white-soggy maceration between the toes are the same. If you have darker skin and you’re scaling, itching, or peeling between the toes, the absence of obvious redness does not rule out athlete’s foot.
Symptoms
- Itching, stinging, or burning — especially after removing shoes and socks
- Peeling, cracking, or scaling skin, particularly between the toes
- Redness and inflammation
- A characteristic musty odor
- Small blisters in some cases
- Thickened, dry skin on the soles in the chronic moccasin pattern
- Sometimes the fungus spreads to the toenails, causing thickening and discoloration (see toenail fungus)
Complications to watch for
Most cases are mild and uncomplicated. But athlete’s foot can lead to several problems worth knowing about — especially if you have diabetes or compromised circulation:
- Bacterial superinfection. Cracked or scratched skin lets bacteria in, and what started as a fungal infection can become cellulitis — a deeper bacterial skin infection that needs prompt antibiotics. Untreated, it can spread quickly.
- “Id” reactions (dermatophytid). An allergic-type rash on the hands or other parts of the body, triggered by your immune response to the foot fungus. The hand rash isn’t itself infected — treating the foot resolves it.
- Spread to the nails. The same dermatophyte can invade toenails, causing the thickening, discoloration, and crumbling of toenail fungus. Once nails are involved, the fungus has a permanent reservoir to keep reinfecting the skin from.
- Spread to other body areas. The same fungus causes jock itch (tinea cruris) and ringworm of the body (tinea corporis) when feet seed other warm, moist areas. Pulling underwear over infected feet is a classic transmission route — put socks on first.
Patients with diabetes, peripheral arterial disease, or immune suppression should treat athlete’s foot promptly rather than waiting it out — these complications are far more common and more dangerous in those groups.
What causes it
The dermatophyte fungi (most commonly Trichophyton rubrum) can survive on damp surfaces for extended periods. You contract it through direct contact with:
- Communal floors (locker rooms, pools, gym showers, dance studios)
- Shared towels, mats, or footwear
- A close contact who is infected
- Soil (rare)
Once on the skin, certain conditions favor establishment:
- Sweaty feet (plantar hyperhidrosis) that stay damp inside shoes for hours
- Closed, non-breathable shoes worn daily
- Synthetic socks that trap moisture
- Walking barefoot in damp public areas
- Weakened immune function (diabetes, certain medications)
- Already-broken skin from blisters or other minor injuries
Treatment options
Most cases respond to over-the-counter topical antifungals. The key is to treat consistently and for long enough — many people stop too soon.
Over-the-counter treatments
- Topical antifungal creams, sprays, or powders containing:
- Clotrimazole (Lotrimin)
- Miconazole (Micatin, Desenex)
- Terbinafine (Lamisil AT)
- Tolnaftate (Tinactin)
- Apply twice daily for at least 2 weeks — often 4 weeks is needed even after symptoms clear
- Treat your shoes — antifungal sprays or powders inside shoes; rotate shoes to let them fully dry between wears
- Change socks if feet sweat through them
- Dry between toes carefully after showering — this is the single most underrated prevention step
When over-the-counter treatment isn’t enough
If symptoms persist after 2–4 weeks of consistent treatment, or if you have a more aggressive form:
- Prescription-strength topicals (econazole, ciclopirox, naftifine)
- Oral antifungal medications (terbinafine or fluconazole) — for stubborn or widespread cases
- Treatment of co-existing conditions — toenail fungus or jock itch often need to be addressed simultaneously to prevent reinfection
- Cultures in unusual cases to confirm the diagnosis
Is it athlete’s foot or something else?
Several conditions look almost identical and get treated wrong for months because they’re mistaken for athlete’s foot.
| Looks like | But it’s actually | How to tell |
|---|---|---|
| Red, itchy, peeling between toes | Foot eczema | Eczema is often symmetrical and may flare with stress or new soaps; tinea pedis is frequently asymmetrical and worsens with sweat. Dyshidrotic eczema (pompholyx) typically lacks the musty odor characteristic of fungal infection unless a secondary bacterial infection occurs. |
| Scaly, thick patches on the soles | Foot psoriasis | Psoriasis has well-defined edges and silvery scale; often involves nails as pitting. Athlete’s foot moccasin pattern is more diffuse without sharp borders. |
| Itchy rash after a new product | Contact dermatitis | Contact dermatitis matches the shape of the trigger (sock seam, shoe lining, lotion). It improves when the trigger is removed. |
| Painful blisters on the arch | Vesicular athlete’s foot OR dyshidrotic eczema | These are genuinely hard to tell apart without testing; a clinician may scrape a blister for fungal microscopy. |
Two-week rule of thumb: if a foot rash hasn’t improved with two weeks of consistent over-the-counter antifungal use, the diagnosis may be wrong. Stop the antifungal and see a clinician for a proper look.
When to see a clinician
Get medical evaluation if:
- Symptoms persist after 2 weeks of over-the-counter treatment
- Signs of bacterial infection appear: increasing redness, warmth, swelling, pus, fever, or red streaks
- The skin is severely cracked, weeping, or painful
- You have diabetes or a compromised immune system — even mild athlete’s foot can become serious
- You’re not sure it’s actually athlete’s foot (eczema, psoriasis, contact dermatitis, and other conditions can mimic it)
Prevention
Once you’ve had it, you’re prone to recurrence. Prevention strategies:
- Dry your feet thoroughly after showering, especially between the toes
- Wear shower sandals in public locker rooms, pools, and shared showers
- Choose moisture-wicking socks (wool, bamboo, synthetic blends) over cotton when feet sweat
- Rotate shoes so each pair has 24+ hours to dry between wears
- Apply antifungal powder in shoes or on feet preventively if you’re prone
- Don’t share towels, socks, or shoes
- Wash feet with soap and water daily; let them air-dry when possible
Living with it
For most people, athlete’s foot is a nuisance more than a serious problem. Catching it early, treating it consistently, and addressing the moisture environment that lets it thrive will resolve the great majority of cases. If you’re getting frequent recurrences, consider whether your shoes, socks, or daily routine are contributing — small environmental changes often outperform stronger medications.
Bottom line
Athlete’s foot is fungal, not a hygiene problem. The most common pattern is between the 4th and 5th toes. Cheap over-the-counter antifungals (clotrimazole, terbinafine) cure the majority of cases when used consistently for 2 to 4 weeks and continued for at least a week after the rash looks gone. The most common reasons it comes back: stopping treatment too early, untreated toenail fungus reseeding the skin, and not treating the inside of the shoes. If you have diabetes, peripheral arterial disease, or compromised immunity, treat athlete’s foot promptly rather than waiting it out.
Frequently asked questions
How long does it take to cure athlete's foot?
Most cases clear with 2–4 weeks of consistent over-the-counter antifungal cream applied twice daily. Stopping treatment as soon as symptoms ease is the most common reason it comes back — keep treating for at least 1 week after the rash looks gone. Stubborn cases may need prescription oral antifungals.
Can athlete's foot go away on its own?
Rarely — the fungus is well-adapted to live on warm, sweaty skin. Without treatment, it usually persists or spreads. The good news: cheap over-the-counter antifungal creams (clotrimazole, terbinafine) cure most cases within a month.
Why do I keep getting athlete's foot?
Recurrence usually means one of three things: the original treatment was stopped too early, the shoes themselves harbor fungus, or there's an untreated source like toenail fungus reinfecting the skin. Treating shoes with antifungal powder and addressing nail involvement breaks the cycle.
Is athlete's foot contagious?
Yes — the fungus spreads through contact with infected skin or contaminated surfaces (locker room floors, shared towels, shower mats). Wearing shower sandals in public wet areas and not sharing footwear or towels reduces transmission.
Should I see a doctor for athlete's foot?
Most cases respond to over-the-counter treatment within a few weeks. See a clinician if it doesn't improve after 2 weeks of consistent treatment, if there's spreading redness or pus (suggesting bacterial infection), or if you have diabetes — even mild athlete's foot in diabetes can lead to serious complications.
Can you wear shoes if you have athlete's foot?
Yes, but keep feet dry — change sweaty socks, rotate shoes between days so each pair fully dries, and use antifungal powder inside shoes. Open shoes (sandals) when possible help airflow. Avoid going barefoot in shared damp areas, where you'd spread it to others.
Sources
Last updated: May 1, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 1, 2026