 or recent nail trauma. Acute cases like this are usually bacterial; chronic cases (weeks to months) are often fungal.](/images/conditions/paronychia.jpg)
Quick answer
Paronychia is an infection of the nail fold — the strip of skin running along each side and the base of a toenail. It’s distinct from an ingrown toenail (where the nail itself digs into skin), but the two often overlap, since an ingrown nail can break the skin and let bacteria in. There are two forms: an acute bacterial infection that develops fast, and a chronic form (usually fungal) that develops slowly over weeks.
The two forms
Acute paronychia
- Develops over hours to days
- Usually bacterial — most often Staphylococcus aureus
- The skin around one nail becomes red, hot, swollen, throbbing
- Pus may collect along the nail edge or under the cuticle
- Pressure-sensitive — even light contact hurts
- Often follows a clear trigger: ingrown nail, hangnail, nail biting, picking, recent pedicure
Chronic paronychia
- Develops over weeks to months
- Usually fungal — most often Candida albicans, sometimes mixed with bacteria
- The cuticle disappears and the skin around the nail becomes swollen and tender without obvious pus
- The nail itself may become discolored, ridged, or distorted
- Far more common on fingers than toes — usually associated with prolonged water exposure (dishwashers, food handlers)
How to recognize it
For the more common acute toe paronychia:
- One toe — usually the big toe — with a red, swollen nail fold
- Pain disproportionate to how the toe looks
- Warmth when touched
- Often a whitish or yellowish bubble of pus visible at the edge
- Throbbing with the heartbeat in advanced cases
- Sometimes fever if the infection is spreading
Why this happens
The cuticle is the seal between the nail plate and the underlying skin. Anything that breaks that seal lets bacteria in:
- Ingrown toenails — pierce the nail fold from inside
- Trauma — stubbing the toe, dropping something on it
- Picking or biting at hangnails
- Aggressive pedicures — cutting the cuticle
- Tight shoes — chronic pressure
- Diabetes — slower healing, higher infection risk
- Immunocompromise — chemotherapy, HIV, transplant medications
When to take it seriously
Most paronychia is a minor problem that resolves with simple home care. But certain features need clinical attention:
- Fever or chills — suggests spreading infection
- Red streaks running up the foot — suggests lymphangitis
- Severe pain despite home care
- Diabetes or peripheral vascular disease — even minor toe infections can become serious quickly
- Spreading redness beyond the nail fold
- Failure to improve in 2–3 days of home care
- Recurrent paronychia in the same toe — usually means an underlying ingrown nail
Treatment
Acute paronychia (early, mild)
If caught early, often resolves with home care:
- Warm soaks in soapy water or saline, 15–20 minutes, 3–4 times daily
- Topical antibiotic ointment (mupirocin or bacitracin)
- Trim shoes that crowd the toe
- Avoid picking or squeezing
- Improvement typically within 2–3 days
Acute paronychia with abscess
If pus has collected, soaks alone usually aren’t enough:
- Incision and drainage by a clinician — small incision releases the pus, dramatic relief
- Oral antibiotics for spreading infection or risk factors (diabetes, immunocompromise)
- Soaks continue after drainage
If an ingrown toenail is the cause
The infection won’t fully resolve until the offending nail edge is addressed:
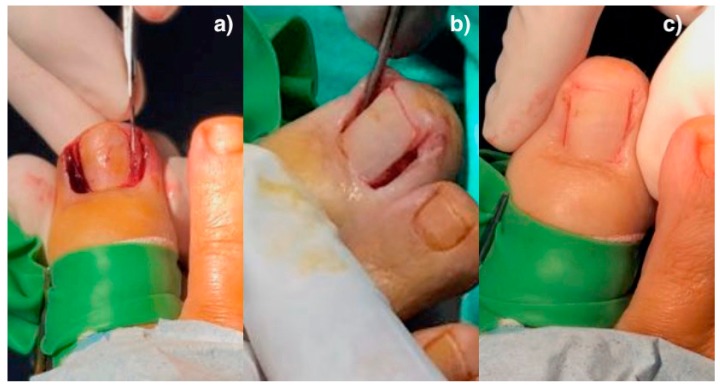
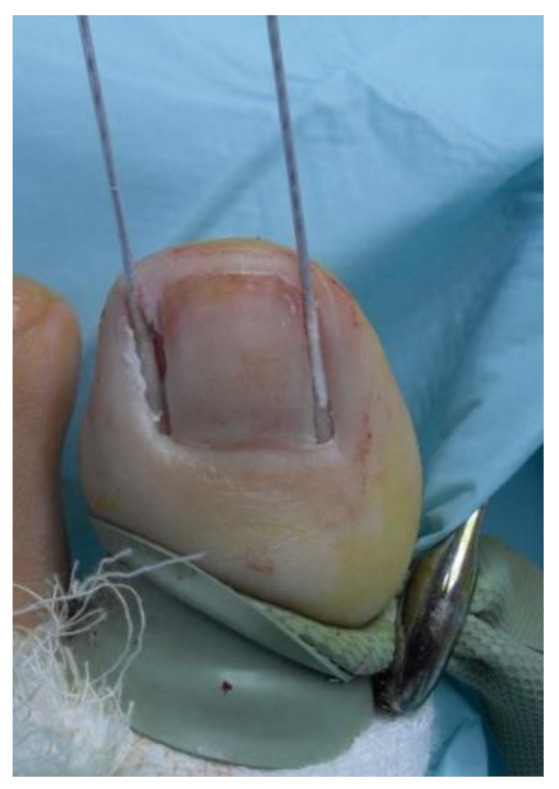
- Partial nail avulsion — the offending edge is removed in a brief in-office procedure
- Matrixectomy (chemical or surgical) — for recurrent cases, the corner of the nail bed that produces the offending edge is permanently destroyed
Chronic paronychia
- Keep the area dry — gloves for wet work, careful drying
- Topical antifungal (clotrimazole, ketoconazole) for Candida-driven cases
- Topical steroid sometimes added for inflammation
- Avoid manicures/pedicures that disrupt the cuticle
- Resolution slow — weeks to months, often with relapse if the underlying triggers continue
Special situations
Diabetic patients
Even minor paronychia in a person with diabetes deserves attention. Diabetic foot infections can progress quickly, and what looks like simple paronychia can be the visible tip of a deeper infection. Lower threshold for clinical evaluation.
Children
Common in toddlers and young children due to nail picking and thumb sucking (when the finger version, “herpetic whitlow,” can mimic bacterial paronychia but is caused by herpes simplex virus and shouldn’t be incised — antiviral therapy is the right approach).
Bottom line
Acute paronychia is one of the most treatable toe problems — most early cases resolve with warm soaks and topical antibiotics. The infection itself isn’t usually the deeper issue: an underlying ingrown toenail is the most common reason these recur. If the same toe keeps getting infected, addressing the nail edge is the durable fix. People with diabetes should treat any toe infection as worth a clinical evaluation rather than home care alone.
Sources
- Muriel-Sánchez JM, Becerro-de-Bengoa-Vallejo R, Montaño-Jiménez P, Coheña-Jiménez M. The Treatment of Ingrown Nail: Chemical Matricectomy With Phenol Versus Aesthetic Reconstruction. J Clin Med. 2020;9(3):845. (CC BY 4.0) ↗
- Muriel-Sánchez JM, Coheña-Jiménez M, Montaño-Jiménez P. Effect of Phenol Application Time in the Treatment of Onychocryptosis: A Randomized Double-Blind Clinical Trial. Int J Environ Res Public Health. 2021. (CC BY 4.0) ↗
Last updated: April 30, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 30, 2026