Quick answer
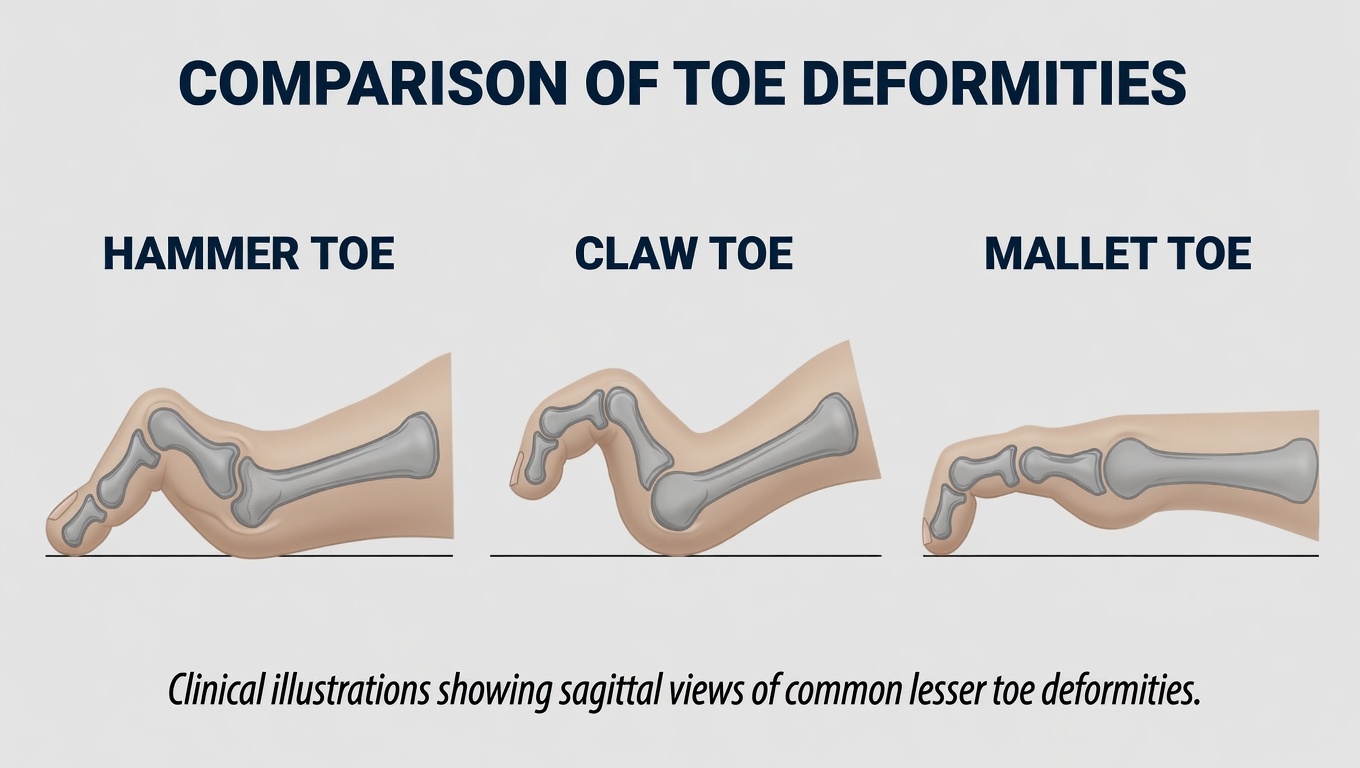
A mallet toe is a toe deformity at the distal interphalangeal (DIP) joint — the joint closest to the toenail. The tip of the toe bends downward, often pressing into the shoe sole and forming a callus or sore. It’s named for the resemblance to a mallet. The other two toe-bending deformities affect different joints: hammertoe bends at the middle joint (PIP), and claw toe bends at multiple joints with the base joint also extended.
How it differs from related deformities
| Deformity | Joint involved | Look |
|---|---|---|
| Mallet toe | DIP only (tip of toe) | Tip points down; rest of toe straight |
| Hammertoe | PIP (middle joint) | Middle joint bent up; tip flat |
| Claw toe | MTP up, PIP down, DIP down | All three joints involved |
Mallet toes most often affect the second toe because it’s typically the longest. Multiple toes can be affected.
Why it develops
- Tight or pointed-toe shoes crush the toe forward, gradually contracting the DIP joint
- A long second toe — repeatedly buckles in shoes
- Tendon imbalance between the long flexor and extensor tendons
- Prior trauma — a stubbed toe or ligament injury at the DIP
- Neuropathy — diabetic patients lose proprioception and develop deformities silently
- Inflammatory arthritis — rheumatoid arthritis classically deforms small toe joints
Early on the deformity is flexible (you can manually straighten the toe). With time it becomes rigid as the joint capsule and tendons contract.
How to recognize it
- Tip of the toe bent downward at the DIP joint
- Callus on the tip of the toe — from pressing into the shoe sole
- Callus on the top of the joint if the bent toe rubs against the shoe top
- Ulcer on the tip in diabetic patients — a serious warning sign
- Pain when shoes are on, less when barefoot
- Difficulty fitting in shoes, especially fashion shoes
Diagnosis
Mallet toe is a clinical diagnosis — visual exam plus tactile assessment of flexibility:
- Flexible mallet toe — can be manually straightened
- Semi-rigid — partial correction
- Rigid — won’t straighten regardless of pressure
X-rays are obtained when surgery is being considered or to evaluate joint condition.
Treatment
Conservative care (flexible mallet toe)
- Wide toe-box shoes — the single most important change
- Mallet toe pads — small foam or silicone pads that hold the toe straight
- Toe sleeves or buddy taping to position the toe and reduce friction
- Pumice or callus reduction — by a podiatrist if calluses are painful
- Stretching and strengthening of the toe muscles
- Custom orthotics — when foot mechanics (long second toe, plantar pressure) are contributing
Diabetic patients
Special caution applies. Pressure ulcers on the tip of mallet toes are a leading cause of diabetic foot infection and amputation. Daily foot inspection, well-fitted shoes, and prompt podiatric care are essential.
Surgery (rigid mallet toe or persistent symptoms)
- Flexor tenotomy — release of the long flexor tendon at the DIP. Often done in office, especially for diabetic patients with tip ulcers
- DIP joint arthroplasty or fusion — for rigid, painful deformities
- Recovery — typically 4–6 weeks of post-op shoe; full recovery 6–12 weeks
Risks of surgical correction
Mallet toe surgery is generally a successful procedure but it is not minor and carries real risks. Reported complication rates for lesser-toe surgery range broadly (roughly 10–30% depending on technique, rigidity, and patient factors). Specific risks include:
- Recurrence of the deformity, particularly in rigid cases or when the underlying cause (long second toe, neuropathy, inflammatory arthritis) continues
- Stiffness of the operated joint — straighter but less mobile
- Floating toe — the operated toe no longer touches the ground
- Overcorrection producing an upturned or hyperextended toe
- Infection — superficial wound infection is common; deep infection or osteomyelitis is rare but serious
- Neurovascular injury — small nerves and arteries to the toe can be stretched or cut, causing persistent numbness, hypersensitivity, chronic pain, or — rarely — vascular compromise of the toe
- Pin problems when temporary K-wires are used (migration, breakage, pin-tract infection, scarring)
- Hardware problems when screws or implants are used (irritation, prominence, breakage, removal surgery)
- Non-union of a fusion — bones fail to grow together
- Persistent or new pain at the operated toe even after technically successful surgery
- Wound healing problems, especially in patients with diabetes, peripheral arterial disease, or who smoke
- Cosmetic dissatisfaction
- Need for revision surgery
- Anesthetic risks common to any surgery
Risks are higher in patients with diabetes, smokers, those with peripheral arterial disease, and patients with neuropathy (where pin or wound problems can go unnoticed and progress quickly).
This page is general educational information and is not a substitute for an in-person evaluation. Anyone considering surgery for mallet toe should have an unhurried in-person consultation with a board-certified foot and ankle surgeon (orthopedic or podiatric) to review their X-rays, the specific procedure proposed, and the full list of risks before deciding.
Bottom line
Mallet toe is the least talked-about of the bent-toe deformities, but it causes a lot of toe-tip pain and shoe-fit trouble. Early flexible mallet toes respond well to footwear changes and padding. Rigid deformities need surgery for reliable correction. In diabetic patients, pressure ulcers on the tip of a mallet toe are a medical urgency, not a cosmetic concern.
Last updated: April 27, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 27, 2026