Urgent — see a clinician today, not next week. Any suspected diabetic foot ulcer — even one that looks small or is painless — needs same-day or next-day evaluation by a podiatrist, primary care physician, urgent care, or emergency department. Diabetic ulcers progress fast, often without pain, and what looks like a callus, a blister, or a small scrape can be hiding much deeper damage. Do not self-treat or “wait and see.” This is the single most important sentence on this page.
What it is
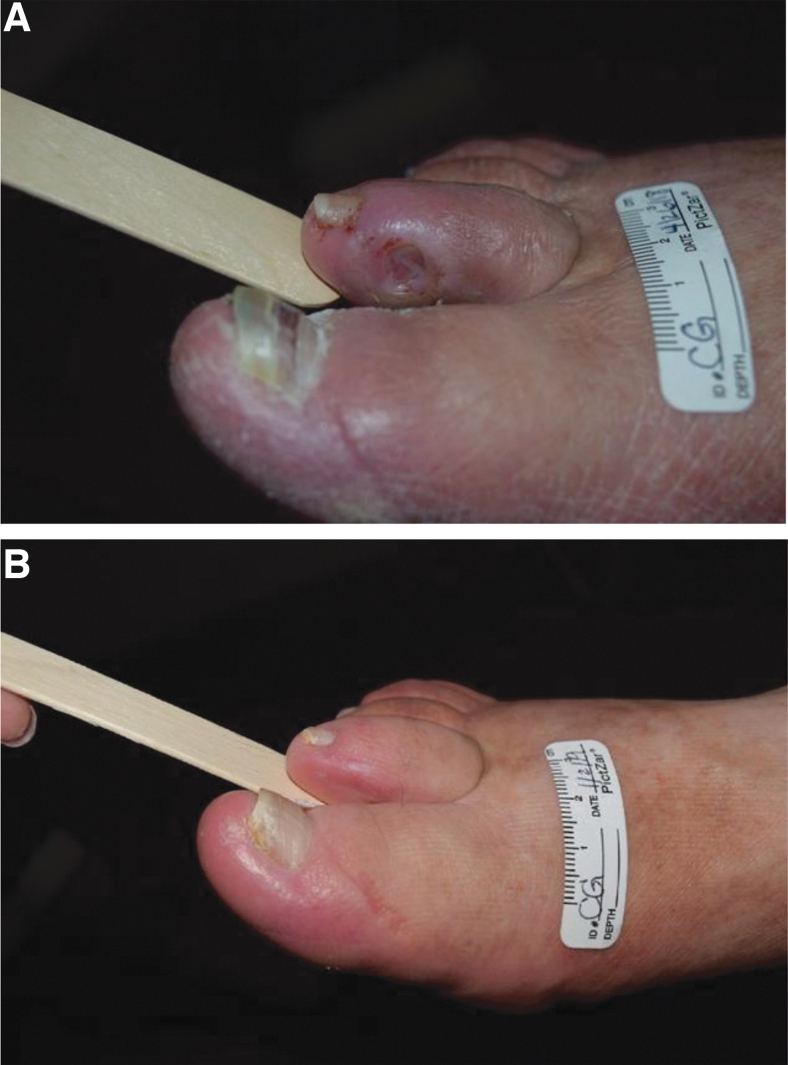
A diabetic foot ulcer (DFU) is an open wound on the foot of a person with diabetes that fails to heal in the normal time frame. They’re most common on the bottom of the foot, particularly under the ball of the foot and big toe, but can occur anywhere — including between toes, on the heel, or under a nail.
DFUs are the leading cause of lower-limb amputation worldwide and a major contributor to hospitalization in people with diabetes. The numbers are sobering: about half of foot ulcers become infected, and a meaningful fraction of those lead to amputation.
But the more important framing: the great majority of DFUs are preventable. The story of a diabetic ulcer almost always starts with a small, unnoticed injury — a blister from new shoes, a stone in a sock, a callus that wore through, a paper cut you’d never feel. The conditions that turn a tiny injury into an ulcer are well-understood. So is what to do about them.
Why diabetes makes this so much harder
Three diabetes-related changes combine to set the stage:
1. Neuropathy — you can’t feel the injury
Diabetic peripheral neuropathy damages the small nerves that supply the feet. The classic pattern is a “stocking” distribution of numbness that starts at the toes and creeps up. Over years, sensation can be reduced to nearly nothing. A sharp object, a hot surface, a stone in a shoe — none register pain. People with significant neuropathy can walk all day on a foreign body or a developing wound without knowing.
2. Poor circulation — wounds don’t heal
Diabetes accelerates peripheral arterial disease. Arteries supplying the legs and feet narrow, reducing oxygen and nutrient delivery to the tissues. A wound that would heal in a week in a healthy person can take months in someone with diabetes — long enough for infection to take hold.
3. Biomechanical changes — high-pressure points
Long-standing diabetes alters foot structure: the small intrinsic muscles weaken, leading to clawed toes; the fat pad under the ball of the foot thins; glycation stiffens collagen, creating limited joint mobility. The result is concentrated pressure on a few spots — exactly where ulcers tend to develop.
Add high blood sugar to the mix, which impairs immune cell function, and the wound that started small spirals into something serious.
Recognizing an ulcer (and a pre-ulcer)
Most DFUs go through a pre-ulcer phase before becoming an open wound. Catching them here makes a huge difference.
Warning signs that warrant prompt evaluation:
- A callus that’s changed — gotten thicker, redder, or developed a darker spot underneath (often pre-ulcerative bleeding). A discrete deep keratotic spot inside a callus — sometimes a porokeratosis — can hide a pre-ulcer; have a clinician inspect anything that looks more than skin-deep.
- A blister in someone with diabetes — even a small one
- Color changes in the skin — redness, blue/purple, blackening
- Cracks in the skin of the heel or between toes
- A small wound that doesn’t seem to be healing
- Drainage through a sock, especially with odor
- Increased warmth in one area of the foot compared to the other side
- An ingrown toenail with surrounding redness
If you have diabetes and notice any of these, call your podiatrist or primary care office the same day. This is not something to “watch and see” for a week.
Severity grading
DFUs are classified using systems like the Wagner or University of Texas classifications. In plain terms:
- Superficial ulcer — limited to the skin, no infection
- Deeper wound — extending into fat or muscle
- Wound with infection — cellulitis, abscess, or deeper tissue infection
- Wound with bone involvement (osteomyelitis) — much more serious
- Gangrene — tissue death, often signaling severe arterial disease
The depth and presence of infection or vascular disease drive treatment decisions.
Treatment
DFUs are a multidisciplinary problem. Effective care typically involves a podiatrist, a primary care doctor (often endocrinologist), and sometimes vascular surgery, infectious disease, and wound care nursing. A coordinated team produces the best outcomes.
The four pillars of treatment:
1. Offloading
The single most important factor. The wound has to be kept off the ground. Options include:
- Total contact cast — the gold standard for plantar (bottom-of-foot) ulcers
- Removable cast walker (CAM boot)
- Surgical shoe with offloading insert
- Wheelchair or crutches for non-weight-bearing
- Custom orthotics for ulcer prevention after healing
2. Wound care
- Debridement — removing dead tissue, usually surgical
- Appropriate dressings — kept moist but not wet; many specialty dressing types depending on wound characteristics
- Regular reassessment — every 1–4 weeks initially
3. Infection control
- Antibiotics when infection is present (oral for mild, IV for severe)
- Cultures to guide antibiotic choice
- Surgical drainage for abscesses
- Hospitalization for severe infections, sepsis, or osteomyelitis
4. Vascular assessment
- Ankle-brachial index (ABI) to screen for peripheral arterial disease
- Vascular consultation for ulcers not healing or with reduced blood flow
- Revascularization (angioplasty, bypass) when indicated to restore blood flow
Adjuncts
- Strict glucose control — high blood sugar impairs healing and immunity
- Nutrition optimization — adequate protein and micronutrients
- Smoking cessation — smoking dramatically worsens healing
- Advanced wound therapies — negative pressure wound therapy, growth factors, skin substitutes for stubborn wounds
Prevention — the most important section
Prevention is enormously effective. The framework comes from international guidelines (IWGDF):
Daily habits
- Inspect your feet every day — top, bottom, between toes. Use a mirror for the soles, or have someone else look. Look for redness, cracks, blisters, color changes, or anything new.
- Don’t go barefoot — even at home. Socks plus slippers minimum.
- Check inside your shoes before putting them on for stones, folded liners, or foreign objects.
- Wash daily with mild soap and warm (not hot) water. Dry carefully, especially between toes.
- Moisturize the dry skin of the heels — but not between the toes (encourages fungus).
- Trim toenails straight across, not too short. If your nails are thick, your eyesight is poor, or you have neuropathy, get them trimmed by a podiatrist.
Footwear
- Always wear shoes that fit properly, with adequate width and depth
- Break in new shoes gradually — wear for 1–2 hours initially, inspect feet afterward
- Replace worn shoes
- For people at higher risk: diabetic / extra-depth shoes with custom inserts, often covered by insurance
Regular checkups
- Annual foot exam at minimum (every 3–6 months for higher-risk people) by a podiatrist or primary care provider
- More frequent visits if you have neuropathy, peripheral arterial disease, foot deformity, or a history of ulcers
Recognize your risk category
The IWGDF risk stratification (a useful framework):
- Very low risk — no neuropathy, no PAD: annual exam
- Low risk — one risk factor: 6–12 month exams
- Moderate risk — two risk factors: 3–6 month exams
- High risk — prior ulcer, amputation, or end-stage renal disease: 1–3 month exams
Your podiatrist can tell you which category you’re in.
When to go to the emergency department (not a clinic)
The clinic is for early concerns. The emergency department is for any of the following — do not wait for a podiatry appointment:
- Fever, chills, or feeling generally unwell with a foot wound
- Red streaks spreading up the foot, ankle, or leg from a wound
- Black, gray, or rapidly darkening tissue (signs of gangrene)
- Foul-smelling drainage
- Severe foot pain that is new or worsening — especially in a foot that previously had no sensation
- A wound that has visibly enlarged in 24 hours
- Pus draining from a foot ulcer
- Swelling and warmth that is spreading rapidly
- Confusion, dizziness, or rapid heartbeat in someone with a foot wound (possible sepsis)
If you cannot get a same-day podiatry or primary-care appointment for any new diabetic foot wound, the emergency department is the appropriate alternative — even if the wound looks small. The cost of a missed early-stage ulcer is often a hospital admission, surgical debridement, or amputation. The cost of an “unnecessary” ED visit is a copay.
Bottom line
A diabetic foot ulcer is a serious problem — but it’s also one of the most preventable serious complications of diabetes. The pieces are:
- Strict glucose control
- Daily foot inspection
- Properly-fitted shoes worn at all times
- Prompt evaluation of any wound, blister, callus change, or color change
- Regular professional foot exams
Following these doesn’t guarantee you won’t develop a problem, but it dramatically reduces the risk and catches issues at the pre-ulcer stage when they’re easy to address.
Frequently asked questions
What does a diabetic foot ulcer look like?
A typical diabetic foot ulcer starts as a small round or oval open sore on a pressure point — most often the bottom of the big toe joint, under the ball of the foot, or on the tip of a toe. The edges may look thickened and callused; the base may be pink (healthier) or yellow/gray (poorer healing). Early ulcers are often painless because diabetic neuropathy has dulled the nerve signal — that's part of why they progress unnoticed. Any open area on the foot of someone with diabetes needs evaluation.
How long does a diabetic foot ulcer take to heal?
With proper treatment, roughly 60–80% of uncomplicated ulcers heal within 12 weeks. Healing depends on three factors: pressure offloading (the ulcer must be removed from weight-bearing), infection control (debridement, antibiotics if infected), and adequate blood supply (which often requires vascular evaluation). Ulcers that haven't healed by 12 weeks have a much higher risk of complications and need specialist input. Some take 6 months or longer; some never fully heal.
Can a diabetic foot ulcer kill you?
Yes, indirectly. Diabetic foot ulcers are the leading cause of lower-limb amputation worldwide, and major amputations carry a 5-year mortality rate of 50–70% — worse than most cancers. The ulcer itself can become infected, the infection can spread to bone (osteomyelitis) and bloodstream (sepsis), and the related cardiovascular disease that drives the underlying neuropathy and arterial insufficiency is also lethal. Early aggressive treatment of any ulcer is the single most important step to prevent these outcomes.
How do you prevent diabetic foot ulcers?
Daily foot inspection (top, bottom, between every toe), well-fitting shoes with smooth seams worn at all times including indoors, regular professional nail and callus care, tight glucose control, not smoking, and routine podiatry visits every 2 to 6 months. People with diabetes plus neuropathy or peripheral arterial disease benefit significantly from therapeutic shoes prescribed by a podiatrist. The single highest-leverage habit is the daily inspection — small problems caught early stay small.
Can a diabetic foot ulcer heal on its own?
Rarely — and trying to wait it out is dangerous. A diabetic foot ulcer represents a failure of the foot's protective system, and without active intervention (offloading, debridement, infection control, vascular assessment), most ulcers either persist, deepen, or become infected. Any new sore on the foot of someone with diabetes is a same-day-or-next-day evaluation, not something to monitor at home. Early treatment doesn't just speed healing — it prevents the progression to amputation.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026