Quick answer
Intoeing (“pigeon-toed”) and out-toeing describe the direction the feet point when a child walks. They can come from the foot itself (metatarsus adductus), the lower leg (tibial torsion), or the hip (femoral version) — and the cause and natural history vary by age and by source. Many cases of childhood intoeing and out-toeing resolve on their own as the child grows. Some do not. Whether your child’s pattern is normal, needs observation, or needs active treatment is a determination for a pediatric foot specialist or orthopedic surgeon — not a decision to make from a website.
Why this happens — three possible sources
The rotation can come from any of three places along the lower limb:
The foot — metatarsus adductus
- Forefoot curves inward while the heel is straight
- Most common in infants — often from intrauterine positioning
- The classic “C-shaped” foot
- Most cases resolve spontaneously in the first 1–2 years
- Flexible cases correct easily with gentle hand pressure
- Rigid cases sometimes need stretching, casting, or rarely surgery
The lower leg — tibial torsion
- The tibia is rotated internally (causing intoeing) or externally (causing out-toeing)
- Internal tibial torsion is the most common cause of intoeing in toddlers and preschoolers
- External tibial torsion is a common cause of out-toeing in older children
- Resolves with growth in most cases — typically by age 6–8
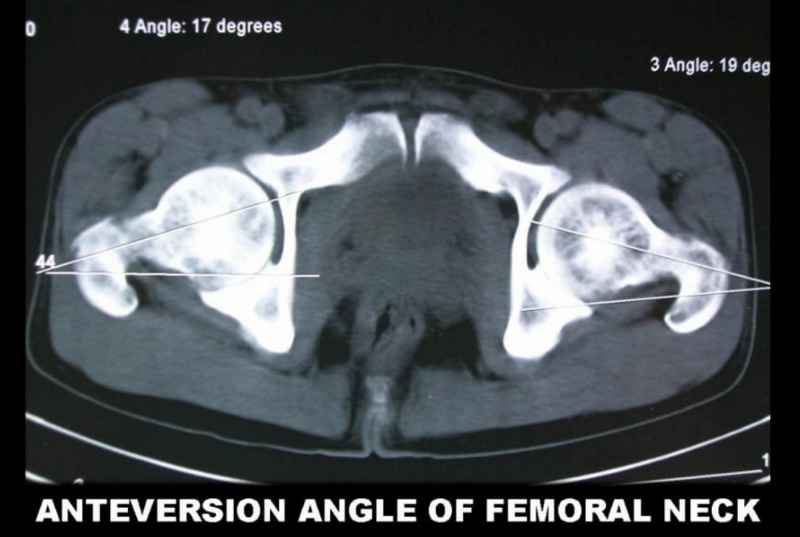
The hip — femoral version
- Femoral anteversion (excessive inward rotation of the hip) — most common cause of intoeing in school-age children
- Femoral retroversion — can cause out-toeing
- Children with femoral anteversion classically sit in the “W” position
- Usually resolves by age 8–10
- Can persist into adulthood in a small percentage
Age-by-age patterns
Infants (0–12 months)
- Most common cause of intoeing: metatarsus adductus
- Most common cause of out-toeing: positional, usually from in-utero position; resolves quickly with weight bearing
Toddlers (1–3 years)
- Most common cause of intoeing: internal tibial torsion
- Bow-legged appearance is also common at this age and is normal
Preschool to early school (3–8 years)
- Most common cause of intoeing: femoral anteversion (the child sits in W)
- Knock-knee appearance is common at this age and is normal
- Rotational profiles change as the child grows
Older children and teens
- Most rotational variations have resolved
- Persistent intoeing or out-toeing may need orthopedic evaluation
How a clinician evaluates this
- Watch the child walk and run — observe foot progression angle
- Examine the foot for metatarsus adductus
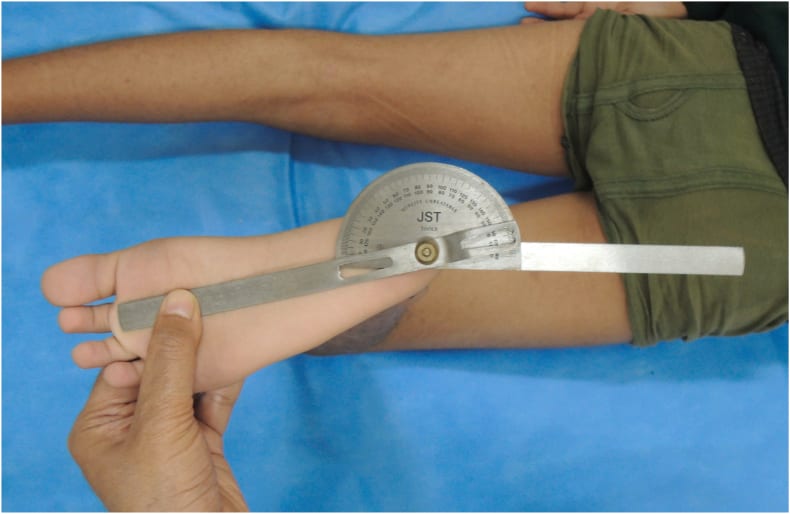
- Check tibial torsion by measuring the thigh-foot angle
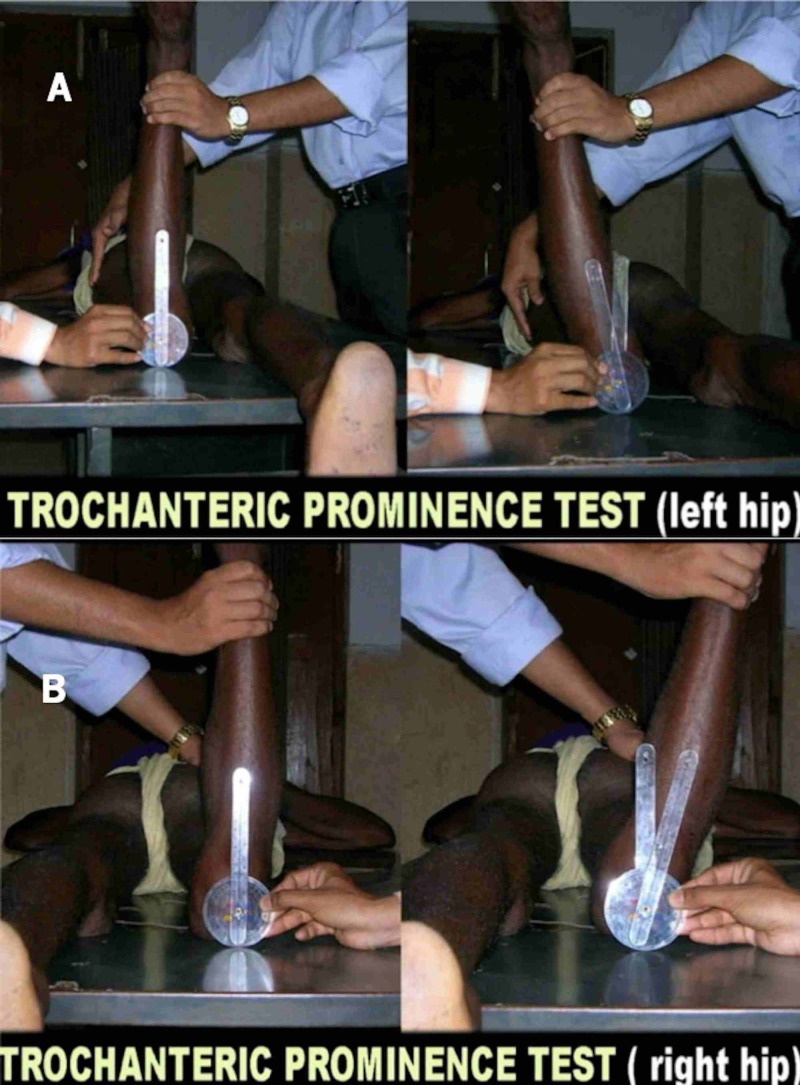
- Check femoral version by examining hip rotation in the prone position
- Look for symmetry — symmetric findings are reassuring; asymmetry sometimes warrants more workup
- Assess function and development — if walking and motor development are normal otherwise, reassurance is usually appropriate
Treatment
The treatment plan depends on the specific cause, severity, age, and how it is progressing, and decisions about whether and how to treat are made by a pediatric foot or orthopedic specialist after an in-person evaluation.
For many children, the appropriate plan after specialist evaluation is observation with periodic re-checks (often every 6–12 months) while growth corrects the pattern. In published evidence, special shoes, corrective braces, twister cables, and routine physical therapy have not been shown to speed up the natural correction of common rotational variations such as internal tibial torsion or femoral anteversion in otherwise healthy children — but the right answer for any individual child still depends on the diagnosis, the severity, associated findings, and the specialist’s judgment.
For some children, active treatment is indicated — for example:
- Rigid or persistent metatarsus adductus may benefit from stretching, serial casting, or rarely surgery
- Severe, functionally limiting tibial torsion or femoral version that does not correct with growth may warrant orthopedic evaluation for derotational osteotomy in older children
- Associated conditions (hip dysplasia, neuromuscular disorders, skeletal dysplasias) need their own targeted treatment
Do not start, stop, or skip treatment based on this page. The decision to observe versus actively treat is a clinical decision that depends on the specific diagnosis and how your child is doing — bring that decision to a pediatric foot specialist, pediatric orthopedic surgeon, or your child’s pediatrician for referral.
When more workup is warranted
Most rotational variations in childhood don’t need imaging or specialist referral. But certain features are worth a clinician’s evaluation:
- Significant asymmetry between the two legs
- Persistent severe deformity at school age
- Pain with walking or activity
- Frequent tripping that’s worsening rather than improving
- Associated developmental concerns — late walking, abnormal motor patterns
- Family history of conditions like skeletal dysplasias or hip dysplasia
- Limp, gait abnormalities beyond simple intoeing
- Persistence into adolescence
These features may indicate a less common but more treatable condition — hip dysplasia, neurological abnormalities, or skeletal dysplasias.
Surgery: rarely indicated
In the very small number of cases that don’t resolve and significantly affect function:
- Femoral derotational osteotomy — for severe persistent femoral anteversion in older children
- Tibial derotational osteotomy — for severe persistent tibial torsion
- These surgeries are uncommon and reserved for clear functional impairment, typically after age 8–10 when natural correction is unlikely
Bottom line
Intoeing and out-toeing in childhood have many possible causes and many possible courses — some resolve naturally with growth, some do not, and a small number signal an underlying condition that benefits from active treatment. The right next step is an in-person evaluation by a specialist — a pediatric foot specialist, pediatric orthopedic surgeon, or your child’s pediatrician — who can examine your child, identify the source of the rotation, look for associated findings, and give you a treatment plan tailored to your child rather than a generic answer. Whether observation, monitoring, casting, bracing, physical therapy, or (rarely) surgery is right for your child is a decision for the specialist after that evaluation. This page is general educational information; your child’s plan should come from their clinician.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026