Quick answer
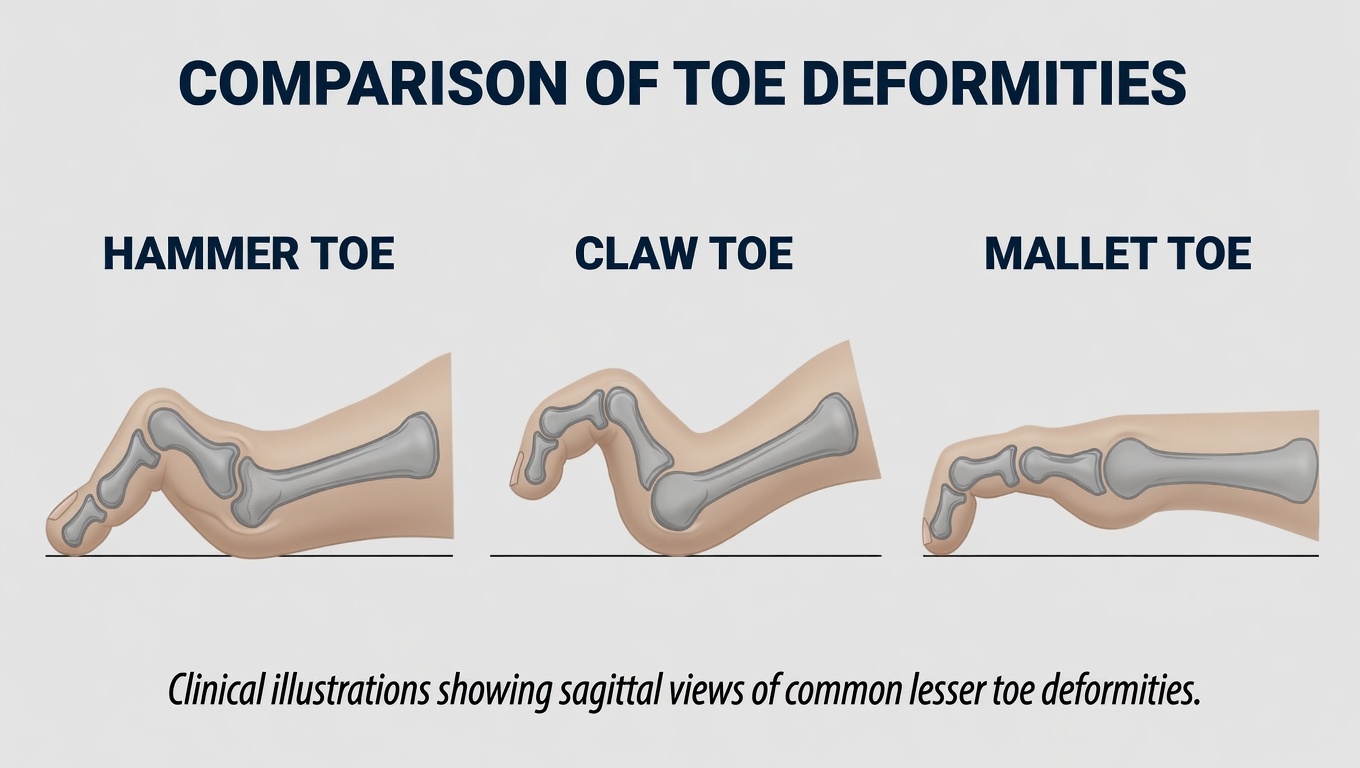
A claw toe is the most extreme of the bent-toe deformities. Three joints in the toe are misaligned at the same time:
- The MTP joint (base of the toe) bends upward
- The PIP joint (middle) bends downward
- The DIP joint (tip) bends downward
The toe takes on a curled “claw” shape. Unlike isolated hammertoe or mallet toe, claw toes typically affect multiple toes at once and often signal an underlying neuromuscular problem rather than just shoe wear.
How it differs from related deformities
- Hammertoe — only the PIP (middle joint) is bent; MTP and DIP are usually straight
- Mallet toe — only the DIP (tip joint) is bent
- Claw toe — all three joints involved
Why it develops
The hallmark of claw toe is muscle imbalance — the small muscles inside the foot (intrinsics) are weak relative to the long muscles in the calf (extrinsics). The intrinsics normally help the toes stay straight; when they’re weak, the long flexors and extensors overpower them and pull the toes into the claw shape.
Common causes include:
- Diabetic neuropathy — the most common cause; intrinsic muscles weaken before the long muscles
- Charcot-Marie-Tooth disease — hereditary peripheral neuropathy that classically produces high arches and claw toes
- Stroke or spinal cord injury
- Rheumatoid arthritis
- High-arch (cavus) foot
- Long-standing tight calf muscles
- Poorly fitted shoes (a contributor in many cases, but rarely the sole cause of full claw toes)
How to recognize it
- Multiple toes bent in a claw shape
- Calluses on top of the PIP joints from rubbing against shoe tops
- Calluses or ulcers on the tips of the toes from pressing into the shoe sole
- Calluses under the metatarsal heads because the toes don’t push off normally
- Difficulty fitting in shoes
- Often accompanies a high arch
In diabetic patients, ulcers at the tips or tops of claw toes are common and can lead to infection.
Diagnosis
- Visual exam — pattern recognition is straightforward
- Assess flexibility — flexible (correctable by hand), semi-rigid, or rigid
- Neurological exam — vibratory sense, monofilament testing, ankle reflexes, lower limb strength
- X-rays — assess joint condition and alignment
- Underlying workup when no clear cause:
- HbA1c to assess for undiagnosed diabetes
- B12 level for neuropathy
- Spinal imaging if hereditary patterns or sudden onset
- Genetic testing for Charcot-Marie-Tooth in clinical cases
A new claw toe pattern in an adult should prompt a search for a neurological cause.
Treatment
Address the underlying cause
When claw toes are a manifestation of diabetes or neuropathy, glycemic control and management of the underlying disease are foundational. The toe deformity itself can’t be fixed without addressing the cause.
Conservative care
- Wide toe-box, deep shoes — the single most important shoe change
- Custom orthotics — to redistribute pressure away from the metatarsal heads and toe tips
- Toe sleeves and pads to protect calluses and reduce friction
- Calf stretching — almost universally part of the cause is calf tightness
- Daily foot inspection in diabetic patients
- Pumice or callus reduction by a podiatrist for painful calluses
Surgery
For rigid claw toes that fail conservative care:
- Flexor tenotomy — release of the long flexor; may help flexible deformities
- Tendon transfer (Girdlestone-Taylor procedure) — reroutes the long flexor to act more like the intrinsic muscles
- PIP joint arthroplasty or fusion — for rigid PIP contractures
- MTP joint procedures — sometimes needed to address the dorsal contracture at the base
- Calf lengthening (gastroc recession) — often combined with toe procedures when calf tightness is contributing
- Recovery — 6–8 weeks in a post-op shoe; full recovery 3–4 months
In diabetic patients with toe ulcers, flexor tenotomy alone often heals the ulcer by relieving tip pressure — a relatively short procedure with a favorable risk profile that can in some cases prevent amputation. The decision still requires in-person evaluation by a foot and ankle surgeon.
Risks of surgical correction
Claw toe surgery is generally a successful procedure but carries higher complication rates than isolated hammertoe or mallet toe surgery because claw toes are usually a manifestation of an underlying neuromuscular disorder (diabetic neuropathy, Charcot-Marie-Tooth, stroke, spinal cord injury, rheumatoid arthritis) — and the underlying nerve disease continues to drive the deformity even after surgery. Reported complication rates for lesser-toe correction range from roughly 10–30%, with recurrence rates noticeably higher when an active neuromuscular cause is present.
Specific risks include:
- Recurrence — the most common complication and the most likely in claw toes specifically, because the underlying neuromuscular cause is not cured by surgery
- Stiffness of the operated toe — straighter but less mobile
- Floating toe — the operated toe no longer touches the ground; particularly common after MTP-level procedures
- Overcorrection producing an upturned or hyperextended toe
- Infection — superficial wound infection is common; deep infection or osteomyelitis is rare but serious, and higher-risk in patients with diabetes
- Neurovascular injury — small nerves and arteries to the toe can be stretched or cut, causing persistent numbness, hypersensitivity, chronic pain, or — rarely — vascular compromise leading to toe necrosis. Diabetic patients with peripheral arterial disease are at higher risk
- Pin problems with temporary K-wires (migration, breakage, pin-tract infection, scarring)
- Hardware problems (irritation, prominence, breakage, need for removal)
- Non-union of a fusion
- Transfer ulceration or pressure — pressure points shift to neighboring toes or the metatarsal head
- Wound healing problems, particularly in patients with diabetes, peripheral arterial disease, or smokers
- Persistent or new pain at the operated toe even after technically successful surgery
- Cosmetic dissatisfaction
- Need for revision surgery
- Anesthetic risks common to any surgery
This page is general educational information and is not a substitute for an in-person evaluation. Decisions about claw toe surgery — particularly in diabetic patients, patients with active neuropathy, or those with peripheral arterial disease — need an unhurried in-person consultation with a board-certified foot and ankle surgeon (orthopedic or podiatric) who has reviewed your X-rays, your underlying medical conditions, and the full list of risks. Surgery on a neuropathic foot is a fundamentally different decision than surgery on a healthy foot, and that judgment is the surgeon’s to make with you.
Bottom line
Claw toes are usually a sign of something larger — most often diabetic neuropathy or another nerve condition. Treatment has two layers: address the systemic cause and treat the mechanical deformity. Conservative measures (shoes, orthotics, calf stretching) help most patients; surgery is reliable for refractory cases. In diabetic patients, claw toes with ulcers are a serious risk for infection and amputation — they warrant prompt podiatric care.
Last updated: April 27, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 27, 2026