
What it is
Hallux rigidus is osteoarthritis of the big toe joint — specifically the first metatarsophalangeal joint (1st MTP), where the big toe meets the long bone of the foot. The cartilage that cushions this joint gradually wears down. Bone spurs (osteophytes) form on top of the joint as the body’s response.
The result is progressive stiffness, especially in the upward-bending direction. Because pushing off requires the big toe to bend up about 65 degrees, even modest stiffness has an outsized effect on walking.
The name reflects the progression:
- Hallux limitus — early stage. The toe still moves but with reduced range and some discomfort.
- Hallux rigidus — late stage. The toe is essentially locked, often with a visible dorsal bump from bone spurs.
It’s distinct from a bunion. A bunion is a sideways deformity (the toe drifts toward the second toe). Hallux rigidus is a vertical-motion problem (the toe can’t bend up). They can coexist, but they’re different problems with different treatments.
Symptoms
Early symptoms:
- Pain at the big toe joint, particularly during push-off when walking or running
- Stiffness when bending the toe upward
- Pain when wearing high heels or stiff dress shoes
- Discomfort during squatting, kneeling, or going up hills
Later symptoms:
- Constant pain even at rest
- A visible bump on top of the big toe joint (the bone spur)
- A dramatically restricted toe — barely able to bend up at all
- Pain that shifts to other parts of the foot, knee, hip, or back as you alter your gait to avoid pushing off the toe
- Numbness or tingling in the big toe (the nerve gets compressed by spurs)
- Calluses on the outside of the foot from walking on the lateral border to avoid the painful joint

What causes it
Most cases are idiopathic — no clear single cause. Contributors include:
- Genetics — foot mechanics that predispose to it are largely inherited
- Foot shape — a long first metatarsal or an elevated first metatarsal can stress the joint
- Previous big toe injury — even a single significant trauma decades earlier
- Repeated minor trauma — common in athletes, particularly soccer players, runners, and dancers
- Inflammatory arthritis — rheumatoid arthritis, gout, and others can damage the joint
- Occupation — jobs requiring extensive squatting, kneeling, or going up and down stairs
Treatment options
Most early-to-moderate cases can be managed without surgery. The goal is to reduce motion at the painful joint and offload the pressure.
Conservative care
- Stiff-soled shoes — surprisingly counterintuitive but very effective. A rocker-bottom shoe or a stiff carbon-fiber insole reduces the bend required at the big toe joint, often dramatically reducing pain.
- Avoid high heels — they force the toe into the painful position
- Custom orthotics with a Morton’s extension — extends rigid support under the big toe to limit motion
- Activity modification — switch from running to cycling or swimming on flare-up days
- NSAIDs — for pain and inflammation, used judiciously
- Ice after activity
- Physical therapy — preserve what motion is left, strengthen surrounding muscles
- Cortisone injection — can provide weeks to months of relief, but repeated injections may accelerate joint damage
Surgical options
When pain limits daily life despite conservative care, several procedures exist depending on the stage. The right operation depends on the severity of the deformity, the condition of the joint surface, the patient’s activity level and goals, and the specific clinical findings — and that decision is one a foot and ankle surgeon (orthopedic or podiatric) makes with you in person after reviewing your X-rays.
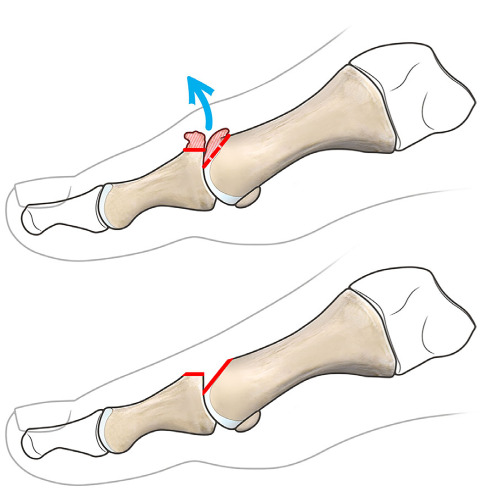
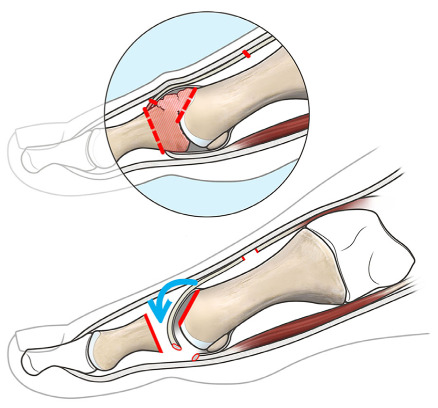
Cheilectomy
Removes the bone spurs on top of the joint and a small wedge of the dorsal first metatarsal head, restoring some upward bending. Most appropriate for early-to-moderate hallux rigidus with reasonably preserved cartilage. Recovery typically 4–6 weeks.
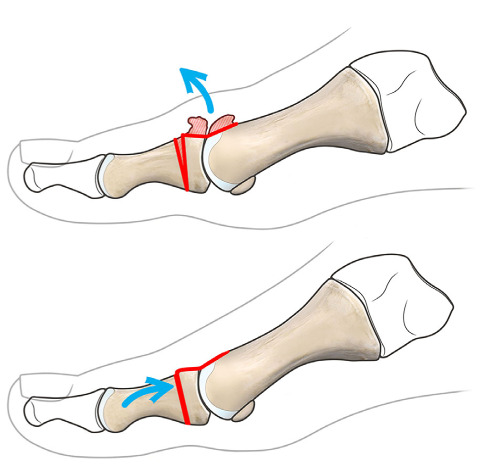
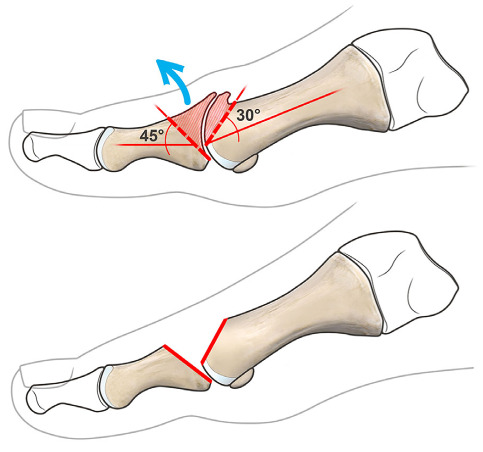
Moberg osteotomy of the proximal phalanx
A dorsal closing wedge osteotomy of the proximal phalanx of the great toe, often combined with a cheilectomy. Effectively shifts available motion toward dorsiflexion (the direction patients need most for walking).
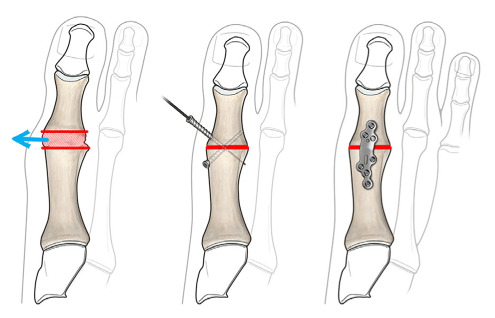
First MTP joint fusion (arthrodesis)
The gold standard for severe hallux rigidus with significant cartilage loss. The two bones are permanently fused in a functional position, eliminating motion at the joint — and therefore eliminating the pain coming from it. Most patients walk and even run normally afterward; high-heeled shoes are no longer comfortable. Highly reliable with very high long-term satisfaction.

Resection arthroplasty (Valenti, Keller variants)
Removes part of the arthritic joint without replacing it. Less reliable than fusion but preserves some motion. Valenti arthroplasty preserves the plantar portion of the proximal phalangeal base, maintaining flexor tendon function while sacrificing extensor structures.
Interposition arthroplasty (Hamilton, MOKCIA variants)
A motion-preserving alternative to fusion in selected patients. A capsular flap (often including the extensor hallucis brevis) is interposed between the bone surfaces after joint debridement.
Joint replacement (synthetic cartilage implant)
Uses an implant to preserve motion at the joint. Synthetic cartilage hemiarthroplasty (e.g., Cartiva) is increasingly used for selected patients but has higher revision rates than fusion long-term. Reserved for carefully selected patients and discussed in detail with a foot and ankle surgeon.
A note on choosing between options
Joint-preserving procedures (cheilectomy, Moberg, interposition arthroplasty) work best before cartilage is fully worn out. Once the joint is end-stage, fusion is the most reliable durable option. The trade-off — motion preserved vs. reliability and durability — is the central decision, and one that depends on age, activity level, and the specific findings on your X-rays.
When to see a clinician
Make an appointment if you notice:
- Pain at the big toe joint that’s persisting or worsening
- Stiffness that’s affecting how you walk
- A growing bump on top of the big toe joint
- Pain in your knees, hips, or back that started around the same time as your toe pain (your gait may be compensating)
- Difficulty finding shoes that don’t aggravate the toe
Earlier evaluation gives you more options. The cheilectomy and other joint-preserving procedures work best before the cartilage is fully worn out.
Living with it
Practical adaptations many people find helpful:
- Reserve high heels and pointy shoes for short occasions, not all-day wear
- Try a carbon-fiber insole — these are inexpensive, available online, and often dramatically helpful
- Look for shoes with a rocker sole — many walking shoe brands now make them
- Don’t push through significant pain — the joint will tell you when it’s had enough
- Consider activity swaps that don’t require big toe push-off (cycling, elliptical, swimming, rowing)
Hallux rigidus is a slowly progressive condition. With sensible management, many people delay or avoid surgery for years — and when surgery is eventually needed, modern techniques are very effective.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026