Quick answer
A toe fracture is a break in one or more bones of the toe (the phalanges). Most occur from stubbing the toe against furniture, dropping a heavy object on the foot, or a sports impact. The good news: most toe fractures — particularly of the smaller toes — heal well with simple home care: buddy taping, stiff-soled shoes, ice, elevation, and time. Big toe fractures and certain other patterns need closer evaluation.
How to recognize a toe fracture
- Sudden pain at the time of the injury
- Swelling of the affected toe
- Bruising — often dramatic, sometimes involving the whole toe and adjacent areas
- Deformity — the toe may look bent or crooked
- Difficulty bearing weight, especially on the front of the foot
- Pain with movement of the toe
- Sometimes a “pop” or “crack” at the time of injury
- Bleeding under the toenail (subungual hematoma) if the toe was crushed
A “stubbed toe” without these features may just be a contusion (bruise) — but with significant pain, swelling, and bruising, a fracture is likely.
When you can manage it at home (probably)
For most lesser toe (toes 2–5) fractures without displacement, home care is appropriate:
- The toe is not significantly deformed
- No open wound at the fracture site
- You can bear weight with some discomfort
- Skin is normal color and the toe has normal sensation
- Pain is bearable with over-the-counter pain medication
- Not in a person with diabetes, peripheral vascular disease, or immunocompromise
If all of these apply, the standard home approach is buddy taping, a stiff-soled shoe, ice, elevation, and over-the-counter pain relief. Most heal in 4–6 weeks.
When to see a clinician
Don’t try to manage at home if any of the following apply:
- Big toe injury — these often need imaging and sometimes surgery
- Open wound with the fracture (open fracture — needs urgent evaluation)
- Obvious deformity — toe pointing the wrong direction or appearing dislocated
- Severe pain not relieved with reasonable measures
- Inability to bear any weight
- Bleeding under the toenail covering more than 25% of the nail — may need drainage and may be associated with fracture
- Cold, blue, or pale toe — possible vascular compromise
- Numbness in the toe
- Person with diabetes, vascular disease, or immunocompromise
- Children — growth plate injuries need careful evaluation
- Symptoms not improving after several days of home care
Special cases
Big toe (hallux) fractures
The big toe bears far more weight than other toes — typically about 40% of the load on the front of the foot. Big toe fractures are different:
- More likely to need imaging for proper assessment
- Displaced or angulated fractures often need reduction (manual realignment)
- Some need casting or a stiff-soled shoe for several weeks
- Significantly displaced or unstable fractures may need surgery with pins or screws
- Recovery longer than for lesser toe fractures
Don’t buddy-tape a big toe fracture and assume it’ll heal on its own.
Sesamoid fractures
The sesamoids are two small bones beneath the big toe MTP joint. They can fracture from impact or stress. These are easy to miss and often confused with sesamoiditis — see the dedicated sesamoiditis guide.
Open fractures
Any fracture with an open wound at the site is a surgical emergency:
- Risk of deep infection
- Need for surgical irrigation and debridement
- IV antibiotics
- Tetanus update
- Often need fixation
Cover the wound loosely with a clean cloth and seek emergency care.
Subungual hematomas
Blood collecting under the nail after a crush injury. If it’s painful and covers a significant portion of the nail, drainage by a clinician (small hole in the nail) provides dramatic relief. Often associated with an underlying tuft fracture of the distal phalanx.
Imaging
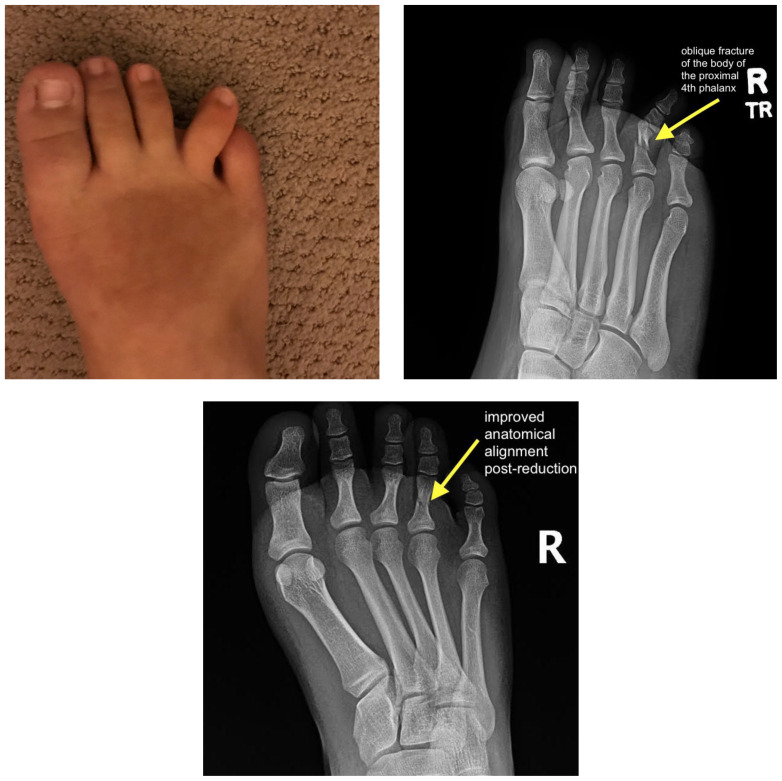
- X-rays of the foot are standard for any suspected toe fracture
- Three views (AP, lateral, oblique) are usually obtained
- Stress views rarely needed
- CT or MRI rarely needed for routine toe fractures; reserved for complex injuries or unclear cases
Treatment
Buddy taping
The injured toe is taped to its uninjured neighbor, which acts as a splint:
- Use medical paper tape or athletic tape
- Place a small piece of cotton or gauze between the toes to prevent skin maceration
- Tape in two places — at the base and at the middle of the toe
- Keep the toes aligned without forcing them
- Replace the tape daily or when it gets wet
- Continue for 3–4 weeks
Stiff-soled shoes
- Limit motion at the fracture site
- Post-op shoes or stiff hiking boots work well
- Wear during all weight bearing for 3–6 weeks
Ice, elevation, NSAIDs
- Ice 15–20 minutes every few hours for the first 48–72 hours
- Elevate the foot above heart level when resting
- NSAIDs for pain (acetaminophen if NSAIDs aren’t appropriate)
Reduction for displaced fractures
If the toe is significantly bent or angulated:
- Manual reduction under local anesthesia (digital block)
- Re-X-ray to confirm alignment
- Splint or buddy tape in the corrected position
Surgery (uncommon)
Reserved for:
- Significantly displaced fractures that can’t be reduced in clinic
- Open fractures
- Big toe fractures with significant displacement or joint involvement
- Multiple fractures or complex patterns
- Fractures with associated dislocation that’s unstable
Procedures involve pins, screws, or plates depending on the pattern.
What to expect during healing
- Pain improves significantly in the first 2 weeks
- Swelling persists for several weeks; bruising may travel down the foot
- Buddy taping and stiff shoe for 3–6 weeks total
- Return to normal shoes when comfortable, usually by 4–6 weeks
- Return to running and jumping typically 6–8 weeks
- Stiffness in the toe may persist for months — gentle range of motion helps
- Some toes heal slightly crooked — usually a cosmetic issue, not functional
Toe dislocations
A toe can dislocate at any of its three joints:
- MTP joint (where the toe meets the foot) — most common, often associated with hyperextension injury
- PIP and DIP joints (the smaller joints in the toe itself)
Dislocations need prompt reduction by a clinician — usually under local anesthesia. After reduction, the toe is buddy-taped or splinted for 2–3 weeks. Recurrent or unstable dislocations may need surgery.
Bottom line
Most toe fractures are simple, self-limited injuries that typically heal well with buddy taping and a stiff-soled shoe over 4–6 weeks. The exceptions matter: big toe fractures, open fractures, dislocations, fractures with significant deformity, and any toe injury in a person with diabetes deserve clinical evaluation. When in doubt — especially for a big toe — get an X-ray rather than assuming the injury will heal itself.
Sources
Last updated: April 30, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 30, 2026