Quick answer
The foot sees a lot of skin problems — some common enough to have their own dedicated guides (plantar warts, athlete’s foot, toenail fungus, corns and calluses, porokeratosis plantaris discreta). This guide covers the lumps, bumps, spots, and unusual skin changes that don’t fit those categories — including pigmented spots, growths, cysts, and lesions that may be malignant such as melanoma and squamous cell carcinoma.
Important — every foot skin lesion should be evaluated in person. Visual diagnosis of skin lesions is unreliable, even for experienced clinicians. Many malignant lesions on the foot — particularly acral lentiginous melanoma and subungual melanoma — look similar to ordinary moles, blood blisters, calluses, or fungal nail changes. The only way to confirm whether a lesion is benign or malignant is an in-person examination and, when indicated, a biopsy. Do not use this page (or any website) to decide a lesion does not need evaluation. If you are reading about a specific spot on your foot, that spot should be examined by a dermatologist, podiatrist, or primary-care clinician — particularly if it is new, changing, bleeding, non-healing, or beneath a toenail. Late diagnosis is the leading reason foot melanoma carries a worse prognosis than melanomas elsewhere.
Lesions commonly seen on the foot — clinical confirmation still required
The categories and descriptions below summarize how various lesions can present clinically. They are not a substitute for in-person diagnosis. Lesions that look textbook-typical can still be malignant, and lesions that look unusual can still be benign — the only way to know is examination and, when indicated, biopsy.
Melanocytic nevi (moles)
Moles are common pigmented spots that can appear on the foot. They typically:
- Appear as flat or slightly raised brown or tan spots
- Have smooth, well-defined edges
- Are symmetric and uniform in color
- Are stable for years — not growing, not changing
- Can be present at birth (congenital nevi) or develop in childhood or adulthood
Important: A mole that looks ordinary on the foot is not necessarily ordinary. Acral lentiginous melanoma can closely resemble a mole, especially in early stages. Apply the ABCDE rule to any pigmented spot (see below). Any mole that is new, changing, growing, becoming itchy, bleeding, or under a toenail should be evaluated by a clinician — visual reassurance from this page or anywhere else is not a substitute for in-person examination.
How dermatologists evaluate foot moles — dermoscopy
When a clinician examines a mole on the foot, they often use a dermatoscope — a handheld magnifying lens with polarized light that reveals patterns invisible to the naked eye. Acral nevi (moles on the palms and soles) follow distinct patterns shaped by the natural ridges and grooves of thick skin:
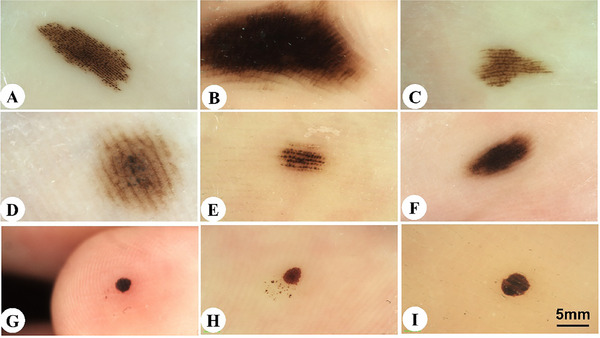
The patterns shown above are all benign. The pattern that raises strong concern for melanoma is the parallel ridge pattern — pigment running along the raised ridges instead of the grooves (essentially the opposite of parallel furrow). Parallel ridge pattern is the dermoscopic hallmark of acral lentiginous melanoma and warrants prompt biopsy.
To the naked eye, every one of these patterns looks like “a brown spot.” A dermatologist with a dermatoscope can distinguish them in seconds. Any new or changing pigmented spot on the foot deserves in-person dermoscopic evaluation rather than visual self-monitoring.
Seborrheic keratosis
Waxy, stuck-on-looking brown or tan growths that appear with age. On the foot they’re less common than on the trunk but do occur:
- Looks like a wart or barnacle — rough, warty surface
- Usually tan, brown, or dark brown
- Stuck-on appearance — as if glued to the skin surface
- Generally non-cancerous — but pigmented lesions that resemble seborrheic keratoses can occasionally be melanoma in disguise (the so-called “melanoma masquerading as seborrheic keratosis”); a clinician should confirm the diagnosis
- Can be removed by a clinician if irritated by footwear (liquid nitrogen, shave excision); a shave biopsy is often appropriate to confirm the diagnosis
Dermatofibroma
A firm, slightly elevated nodule — most common on the lower legs but can appear on the foot:
- Usually pinkish, tan, or brown
- Firm and rubbery to the touch
- The classic dimple sign: pinching the overlying skin makes it dimple inward
- Typically non-cancerous — arises from fibrous tissue in the dermis. However, dermatofibrosarcoma protuberans and other fibrohistiocytic tumors can mimic a dermatofibroma; a clinician should confirm the diagnosis, especially for a larger, atypical, or growing lesion
- Stable, asymptomatic dermatofibromas are often left alone after a clinician confirms the diagnosis; lesions that are painful, growing, or atypical warrant biopsy
Epidermal inclusion cyst (keratin cyst)
A round, moveable lump just under the skin, filled with soft keratin material:
- Common on the plantar surface (sole), sometimes from a previous injury that buried skin cells
- Smooth, dome-shaped, skin-colored or yellow-white
- Can enlarge slowly over time
- If it ruptures, can cause a localized inflammatory reaction (red, painful, swollen — often mistaken for infection)
- Typically non-cancerous, but other deeper foot masses (ganglion cysts, lipomas, soft-tissue tumors, sarcomas) can present similarly; imaging or biopsy is sometimes needed to confirm the diagnosis. Any firm, rapidly enlarging, painful, or atypical foot mass warrants clinical evaluation
- Treated by excision when it causes problems
Pyogenic granuloma
A bright red, rapidly growing vascular lump that bleeds easily:
- Often appears after minor trauma (splinter, thorn, cut)
- Grows within days to weeks — bright red, friable, often looks alarming
- Bleeds with minimal contact
- Typically non-cancerous despite the dramatic appearance — but amelanotic melanoma (pigment-free melanoma) and other vascular tumors can present identically as a rapidly growing, bleeding red nodule. Any rapidly growing, bleeding lesion on the foot must be examined and biopsied — visual diagnosis is unreliable for this presentation in particular
- Treatment is by a clinician — silver nitrate cautery, shave excision, or laser, typically with histopathologic examination of the removed tissue
- Can recur if not fully removed
Talon noir (black heel)
A cluster of small dark spots on the heel, typically in athletes:
- Caused by shearing forces during sport — the heel skin compresses and tiny blood vessels rupture
- Painless dark spots on the heel or lateral foot
- Common in basketball, tennis, soccer players
- Important — talon noir closely mimics melanoma, and the only reliable way to distinguish them is dermoscopy and, when in doubt, biopsy. The classic teaching that talon noir “pares down” with scraping is suggestive but not definitive. Do not assume a dark heel spot is talon noir without a clinician confirming the diagnosis, particularly if the spot does not fade over a few weeks of reduced activity, is not clearly tied to a specific sport-related shear injury, or has any irregular features
- When the diagnosis is confirmed by a clinician, talon noir typically resolves on its own as new skin grows out

Subungual hematoma (blood under the nail)
Blood collecting under a toenail after trauma:
- A dark brown or black area under the nail, often painful initially
- Common after a dropped object on the toe, tight shoes, or repetitive microtrauma in runners (“runner’s toenail”)
- Important — subungual hematoma can be visually indistinguishable from subungual melanoma, particularly when the patient does not recall the inciting trauma. The classic teaching that hematomas grow out with the nail is true on average but takes weeks to months to confirm — and during that window a melanoma can progress. Any new dark discoloration under a toenail should be evaluated by a clinician, even when there is a plausible trauma history. Features that make melanoma more likely include: pigment that does not move distally as the nail grows, pigment that extends onto the cuticle or surrounding skin (Hutchinson’s sign), a single nail involved without trauma history, or a streak that widens over time
- A clinician can drain a true acute hematoma to relieve pain — see the subungual hematoma page for the trephination procedure and recovery timeline


Images: Puente et al., Cureus, 2025 (CC BY 4.0).
Video — trephination of a subungual hematoma. A clinician uses a heated cautery to make a small hole through the nail plate, releasing the trapped blood and immediately relieving pressure. Video: Puente et al., Cureus, 2025 (CC BY 4.0).
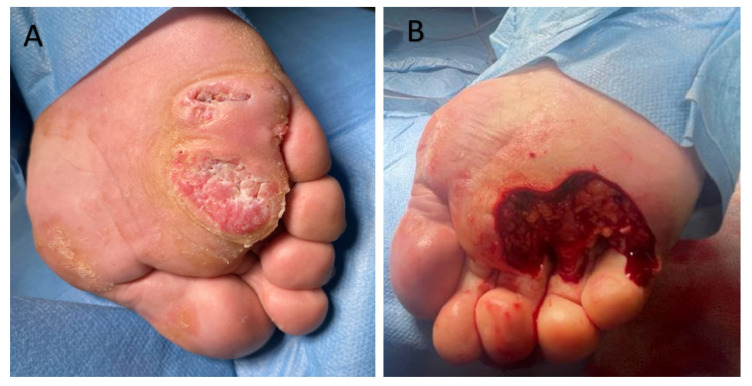
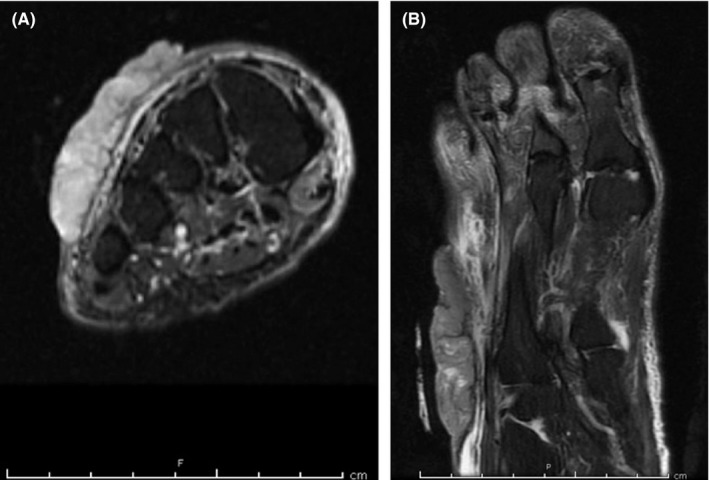
Glomus tumor
A rare, painful benign tumor of the glomus body (a small arteriovenous structure in the nail bed):
- Most common under the fingernail, but occurs in the toe
- Classic triad: severe pain, point tenderness, and cold sensitivity
- The pain is often out of proportion to the lesion’s size
- Treated surgically — excision is curative

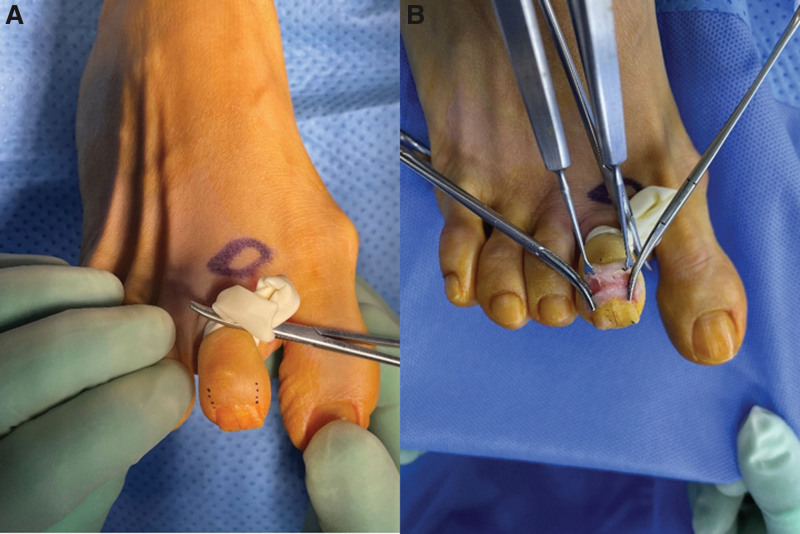
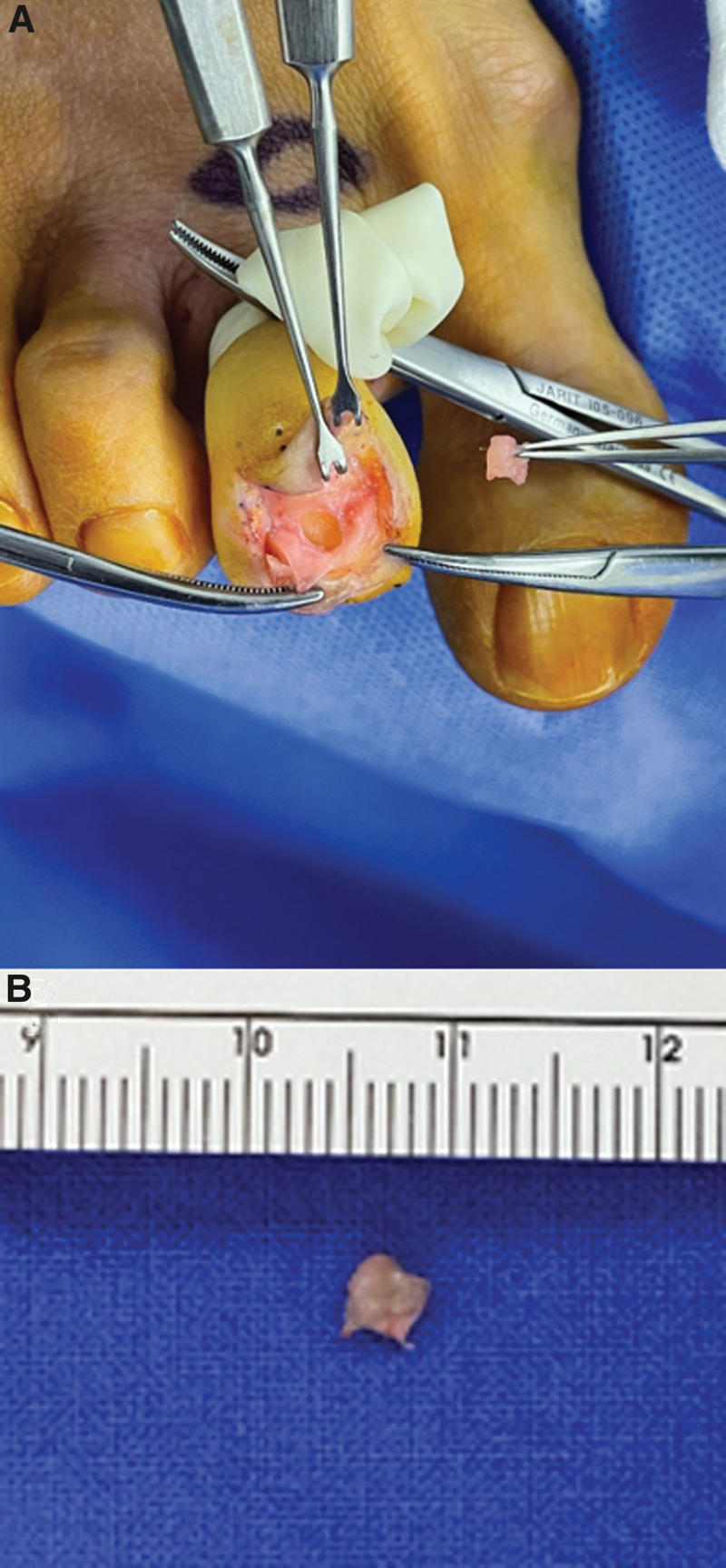
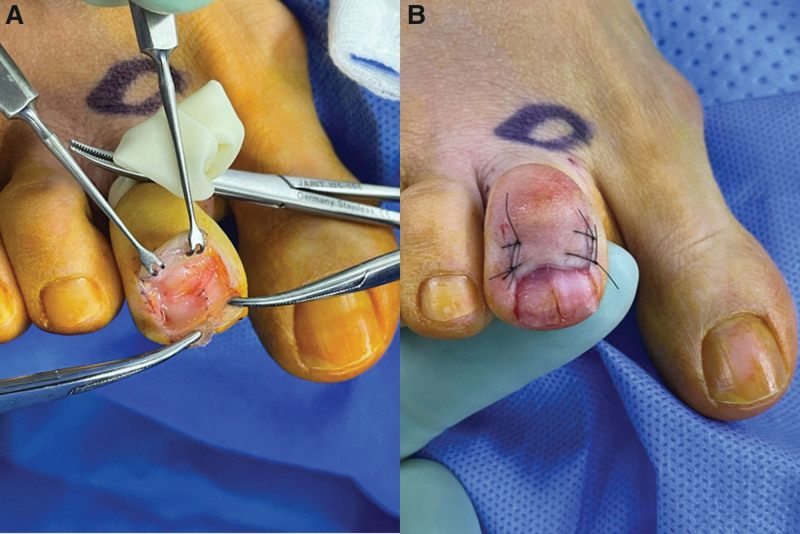

Subungual glomus tumor of the second toe — clinical appearance, imaging, and surgical outcome from a published case. Note the subtle nail deformity in the early views and the preserved nail after excision. Images: Lin et al., World J Clin Cases, 2024 (CC BY 4.0).
Cutaneous horn
A hard, cone-shaped outgrowth of compacted keratin, protruding from the skin:
- Looks like a small animal horn
- Can arise from benign or premalignant/malignant base tissue
- Always warrants biopsy of the base — the overlying horn itself is just keratin, but the underlying process could be a wart, actinic keratosis, SCC, or benign keratosis
Malignant skin lesions
Acral lentiginous melanoma (ALM)
The most important malignant lesion on the foot — and the most often missed.
What it is: A form of melanoma that develops on the soles, between the toes, or under the nails. Unlike other melanomas, it’s not strongly related to sun exposure, which is why it can appear in places that rarely see the sun — including the bottom of the foot.
Why it matters:
- Frequently caught late — the foot is rarely inspected
- The spots look benign and develop slowly
- Late diagnosis is the main reason ALM has a worse prognosis than other melanomas
- The most common type of melanoma in people of African, Asian, and Hispanic descent
- Affects all skin tones equally — it is not a “fair skin only” cancer
On the sole or between toes:
- A new dark spot that wasn’t there before
- An existing spot that’s changing — color, size, shape, borders
- Asymmetric with irregular borders
- Multiple colors within the spot (brown, black, pink, blue, white)
- Larger than ~6 mm (pencil eraser)
Under a toenail (subungual melanoma):
- A dark band running lengthwise under the nail (longitudinal melanonychia)
- A brown or black streak that’s getting wider
- Pigment that extends onto the cuticle or surrounding skin (Hutchinson’s sign — very concerning)
- Nail destruction, splitting, or separation
- Single nail involved — multiple dark nails are usually benign; one streak in one nail that’s growing needs evaluation
Evaluation: Dermoscopy by a dermatologist; biopsy if suspicious; wide local excision with sentinel lymph node consideration if confirmed.
Squamous cell carcinoma (SCC)
The second most common skin cancer overall, and fully capable of arising on the foot:
- Can appear as a rough, scaly, red or pink patch that doesn’t heal
- Sometimes a firm nodule or ulcer with raised edges
- Often in areas of chronic irritation — old wounds, scars, or areas with long-standing inflammation
- Bowen’s disease (SCC in situ) appears as a persistent, flat, scaly, reddish plaque
- SCC on the foot is sometimes called verrucous carcinoma when it grows in a warty pattern — can be mistaken for a plantar wart for years
- Can spread to lymph nodes if neglected; foot SCCs are sometimes caught late due to diagnostic delay
- Treatment: surgical excision with clear margins; advanced cases may need lymph node evaluation
Basal cell carcinoma (BCC)
The most common skin cancer overall, but rare on the sole (which receives minimal UV):
- More common on the dorsum (top) of the foot than the sole
- Classic appearance: pearly, translucent papule with rolled borders and small blood vessels
- Can ulcerate (“rodent ulcer”)
- Rarely spreads but locally destructive if neglected
- Treatment: excision, Mohs surgery, or topical therapy depending on size and location


Large fungating basal cell carcinoma of the foot dorsum — preoperative appearance, surgical excision, and reconstruction. This is an unusually large example (8 × 8 cm) that grew over time without evaluation; most BCCs are caught much smaller. The dorsum (top) of the foot is the typical location because it gets more sun exposure than the sole. Images: Mamtani et al., Clin Case Rep, 2018 (CC BY 4.0).
A vascular tumor most commonly seen in immunocompromised patients (HIV/AIDS, transplant recipients):
- Purple, brown, or red plaques or nodules on the foot and lower legs
- Common on the soles
- Can be first sign of unrecognized HIV in some patients
- Treatment: depends on extent of disease and immune status — may include antiretroviral therapy, chemotherapy, radiation
The ABCDE rule — applied to the foot
Use this for any pigmented spot:
- Asymmetry — one half doesn’t match the other
- Border — irregular, ragged, notched, or blurred edges
- Color — multiple shades; especially concerning with black, white, blue, or red within the same lesion
- Diameter — larger than 6 mm (pencil eraser); though melanomas can be smaller
- Evolving — changing in size, shape, color, or any new symptoms (bleeding, itching)
Any “E” alone — a lesion that’s changing — is reason for evaluation regardless of other features.
When a foot skin lesion needs prompt evaluation
See a dermatologist for:
- New or growing pigmented spot on the foot
- Dark streak under a toenail — especially if getting wider, or if pigment spreads to the cuticle
- Lesion that bleeds without obvious trauma
- Non-healing sore or ulcer on the foot (think SCC, especially in an old scar or chronic wound)
- Red, rapidly growing vascular lump (pyogenic granuloma — benign but needs treatment)
- Any lesion you’re uncertain about
- Strong family history of melanoma — worth a dermatology consult even without a specific concerning lesion
Don’t wait months to see if it “goes away.” Most of these are benign, but the ones that aren’t are much more treatable when caught early.
Self-screening habit
The foot is one of the least-inspected parts of the body — which is why malignant lesions here are often caught late. A simple monthly habit:
- Inspect your soles, between the toes, and all toenails
- Use a mirror or ask someone to check the soles if you can’t see them clearly
- Photograph any spots you’re watching and compare at 4–6 weeks
- Don’t dismiss “weird” spots because they’re in a hard-to-see location
Bottom line
Visual diagnosis of foot skin lesions is unreliable — the only way to know what a lesion actually is, is in-person evaluation by a clinician and biopsy when indicated. Acral lentiginous melanoma and subungual melanoma can closely resemble ordinary moles, blood blisters, calluses, fungal nail changes, and pigmented streaks — and they carry a worse prognosis than other melanomas precisely because they are caught late. Set the bar low. Any new, changing, bleeding, non-healing, or otherwise unusual lesion on the foot — including under a toenail — warrants in-person evaluation. A dermatologist or podiatrist examination is brief, low-risk, and the only reliable way to rule out malignancy. Do not use this page (or any other website) to talk yourself out of a clinic visit.
Sources
- Cui Z, Wu J, Fang L, Ren C. Dermoscopic Features of Plantar and Palmar Melanocytic Nevi in Children. Skin Res Technol. 2026. (CC BY 4.0) ↗
- Choudhury S, Mandal A. Talon Noir: A Case Report and Literature Review. Cureus. 2023;15(3):e35905. (CC BY 4.0) ↗
- Puente RC, Diaz de León Guzmán AI, De León Puga LS, Rosales Verduzco PV, Tovar Garcia A. Subungual Hematoma: Insights From a Clinical Case Study. Cureus. 2025;17(5):e84493. (CC BY 4.0) ↗
- Lin Y-L, Chen H-Y, Chen W-J, Lin Y-C. Nail-preserving excision of glomus tumor in the second toe: Case report and literature review. World J Clin Cases. 2024. (CC BY 4.0) ↗
- Costache M, Sajin M, Lazaroiu AM, et al. Squamous Cell Carcinoma and Its Rare Variant, Carcinoma Cuniculatum. (MDPI), 2025. (CC BY 4.0) ↗
- Mamtani S, Aljanabi NM, Gupta Rao N, Aldana PC, Pulumati A. Large fungating basal cell carcinoma of the dorsum of the foot: A case report. Clin Case Rep. 2018;6(11):2169-2172. (CC BY 4.0) ↗
Last updated: April 30, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 30, 2026