Quick answer
A plantar wart is a virus-caused growth on the bottom of the foot. The virus is HPV, picked up through tiny breaks in the skin — usually from walking barefoot on damp public surfaces. Most go away on their own, but they can hurt and spread, so treatment is often worth it.
Important — make sure it’s actually a wart first. Several things on the bottom of the foot can look like plantar warts but aren’t: a callus, porokeratosis plantaris discreta (PPD), a foreign body (splinter, hair), a pressure ulcer hidden under thick skin, or rarely a melanoma or squamous cell carcinoma. Don’t apply salicylic acid to a lesion you haven’t had confirmed. A clinician can usually tell the difference in seconds. This matters most in people with diabetes, peripheral neuropathy, or poor circulation — get any new lesion on the sole evaluated before treating.
How to recognize one
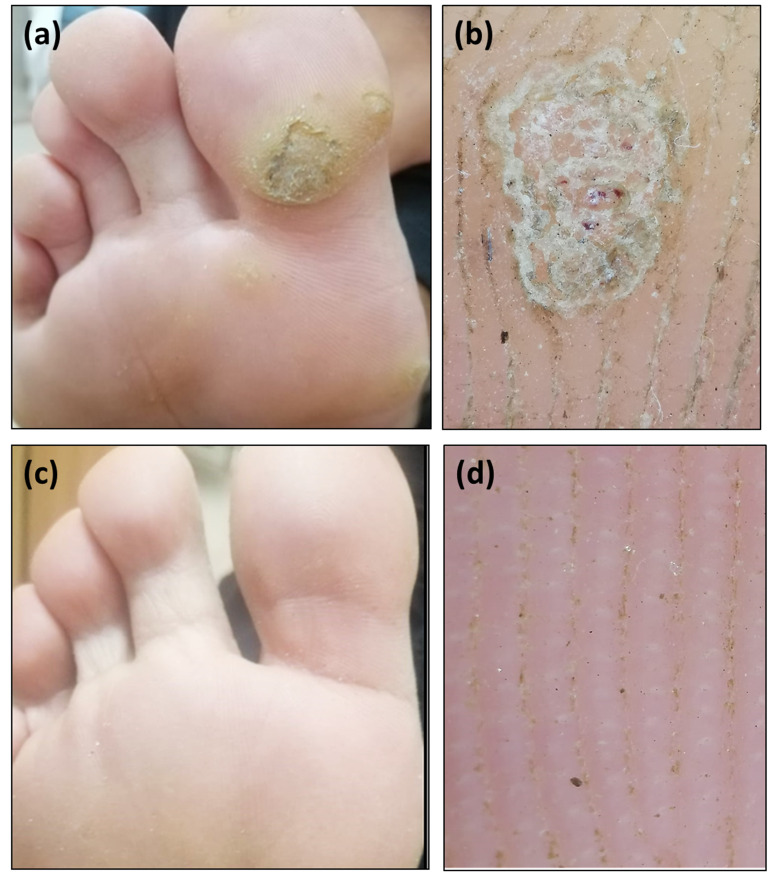
- Small, rough, grainy patch on the sole of the foot
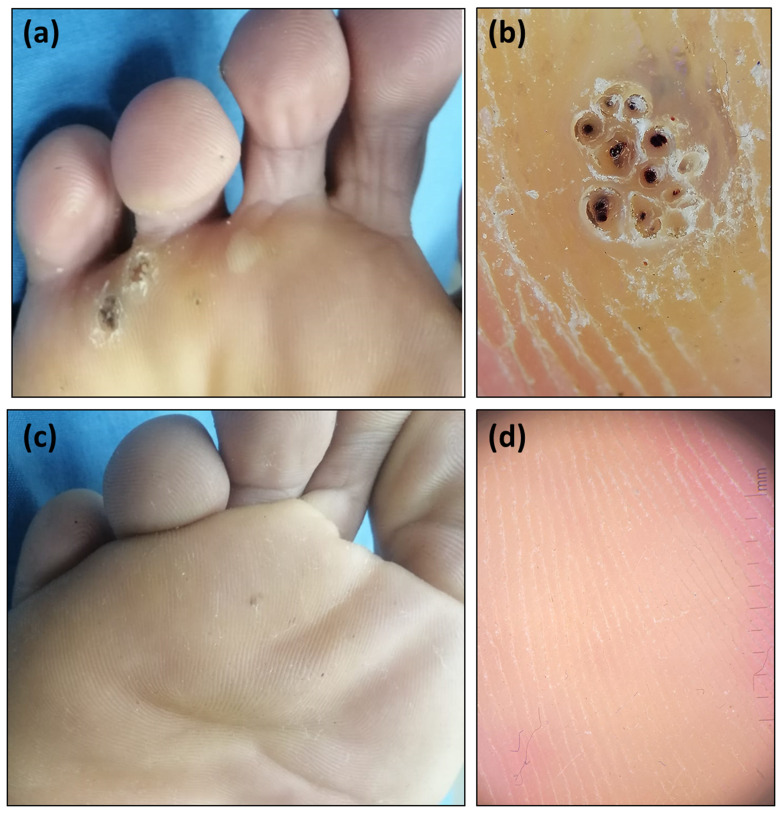
- Tiny black dots within the wart (clotted blood vessels — a hallmark)
- Pain when squeezed from the sides — but less when pressed straight down
- Feels like stepping on a pebble
- May be a single wart or a cluster (“mosaic warts”)
- Disrupts the normal skin lines (calluses don’t)
A callus and a plantar wart can look similar. The black dots and the side-squeeze test are the easiest way to tell them apart.
What causes it
Plantar warts are caused by the human papillomavirus (HPV) — specifically strains that target tough, hairless skin. The virus enters through:
- Tiny cracks or cuts in the skin (often invisible)
- Walking barefoot on contaminated surfaces — pool decks, locker rooms, shared showers, hotel bathrooms
- Direct contact with someone else’s wart
You can also spread your own warts to other parts of your foot by scratching or picking.
Treatment options
About 2 in 3 plantar warts resolve on their own within 2 years — the immune system eventually catches up. But waiting it out isn’t always the right call, especially if the wart is painful or growing.
Try at home first
- Salicylic acid (40% patches or 17% liquid) — apply daily for 8–12 weeks. Soak the foot first, then very gently exfoliate the surface with a pumice stone, apply, cover. The most evidence-based home treatment.
- Duct tape — covering the wart with duct tape between treatments may help (mixed evidence; safe to try)
- Don’t pick or cut — spreads the virus and risks infection
Don’t try home treatment if you have:
- Diabetes — salicylic acid can damage healthy skin and create a wound
- Peripheral neuropathy or any condition that reduces sensation in your feet — you can’t reliably tell when filing is causing damage
- Poor circulation or peripheral arterial disease — wounds are slow to heal
- A weakened immune system
See a podiatrist for in-office treatment instead.
When over-the-counter treatment isn’t enough — see a clinician
- Cryotherapy (liquid nitrogen) — done in-office, usually 3–6 sessions every 2–4 weeks
- Stronger topical agents (cantharidin, prescription-strength salicylic acid)
- Immunotherapy (squaric acid, imiquimod) — for stubborn or multiple warts
- Laser treatment — for resistant cases
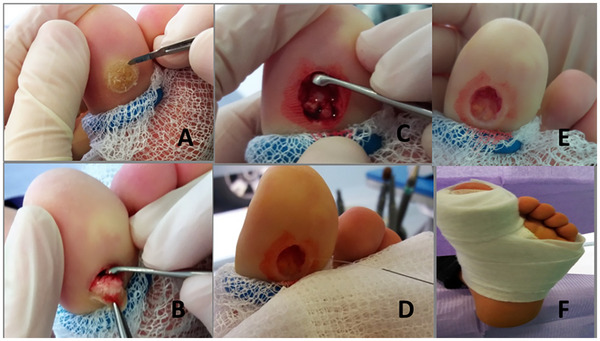
- Surgical removal — last resort due to scarring risk
When to see a clinician
Same-day evaluation for:
- A wart-like lesion that is bleeding, rapidly growing, or painful out of proportion to its appearance — these features can suggest verrucous carcinoma (a slow-growing form of squamous cell carcinoma that can be mistaken for a stubborn plantar wart for months or years) or other skin malignancy
- Any signs of infection — spreading redness, warmth, pus, fever, or red streaks running up the foot
- Any foot lesion in a person with diabetes, peripheral neuropathy, peripheral arterial disease, or a weakened immune system — even if it looks “just like a wart”
Standard appointment for:
- Confirming the diagnosis before starting any treatment
- Pain that limits walking or activity
- A wart that is growing or new lesions appearing
- No improvement after 2–3 months of home treatment
- Multiple warts or recurrent warts
Prevention
- Wear shower sandals in public locker rooms, pools, gyms, hotel bathrooms
- Don’t share towels, socks, or shoes
- Keep feet dry — change wet socks
- Don’t touch other people’s warts (or your own with bare hands)
- Cover existing warts with a bandage when going to the pool or gym to reduce spread
Sources
- Khattab F, Essam R, Elhadidy RF, Anis N. Intralesional combined digoxin and furosemide versus intralesional 5-fluorouracil for the treatment of recalcitrant plantar warts: a prospective, randomized study. Arch Dermatol Res. 2024. (CC BY 4.0) ↗
- Chiva Miralles MJ. Surgical Excision of Plantar Wart. Skin Res Technol. 2026. (CC BY 4.0) ↗
Last updated: April 30, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 30, 2026