Quick answer
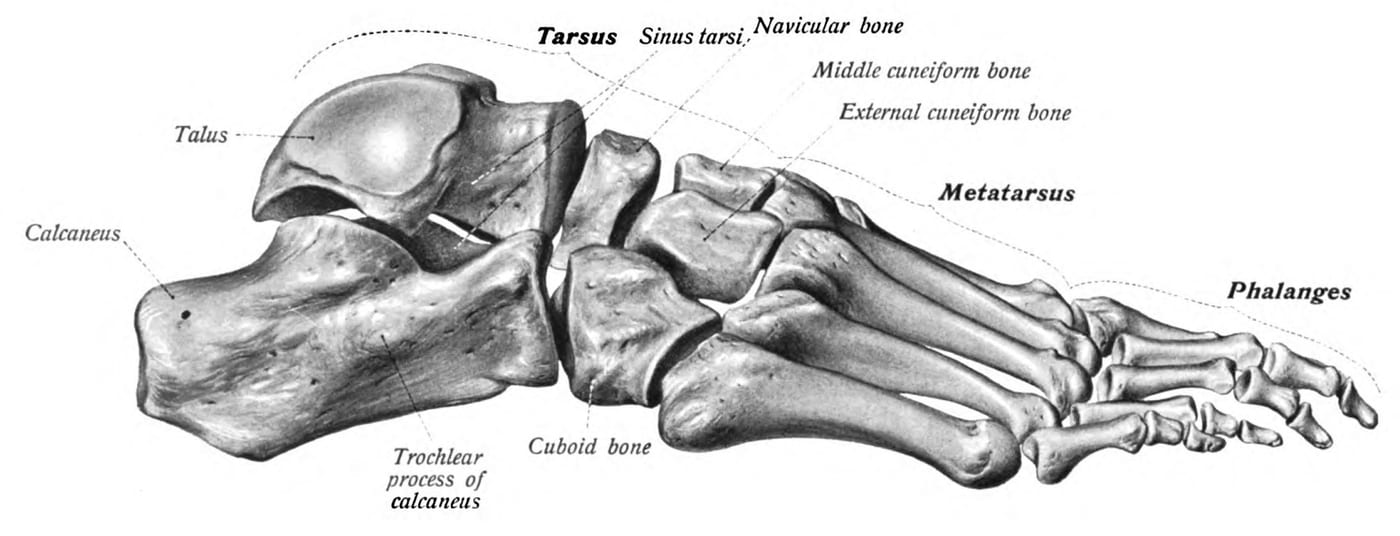
The sinus tarsi is a small bony tunnel on the outside of the foot, just in front of the lateral ankle bone (lateral malleolus). It contains ligaments, fat, and small nerve endings — and when these tissues become inflamed or damaged, you get sinus tarsi syndrome: persistent pain in this exact spot, especially when standing on uneven ground or rolling the foot inward. It’s most often a sequel to an ankle sprain that didn’t fully heal, but it also develops in people with flat feet because of the abnormal position of the hindfoot.
What’s actually inside the sinus tarsi
The sinus tarsi is a roughly cone-shaped opening between the talus and calcaneus. Inside it sit:
- The interosseous talocalcaneal ligament — a key stabilizer of the subtalar joint
- The cervical ligament — another subtalar stabilizer
- Fat and synovial tissue
- Branches of nerves and small blood vessels
Damage or inflammation of any of these structures — especially the ligaments — produces the syndrome.
Why it hurts
Two main pathways lead to sinus tarsi syndrome:
- After an ankle sprain — when the ankle rolls inward (inversion sprain), the talus and calcaneus shift in a way that strains the sinus tarsi ligaments. Most sprains heal, but in a fraction of cases the sinus tarsi tissues remain inflamed or scarred, and the joint feels chronically unsettled.
- Flatfoot mechanics — when the arch collapses, the heel tilts outward (valgus) and the talus drops inward, closing down the sinus tarsi space. The tissues inside get pinched. This is why sinus tarsi syndrome is common in adult-acquired flatfoot from posterior tibial tendon dysfunction.
Less often it’s caused by inflammatory arthritis, infection, or a mass within the sinus tarsi.
How to recognize it
- Pain in the “soft spot” just in front of and below the lateral ankle bone — a very specific location patients can usually point to with one finger
- Worse on uneven ground, walking on slopes, or running
- Worse with prolonged standing
- Better with rest and supportive shoes
- Often a sense of hindfoot instability — feeling like the foot might give way even though the ankle isn’t actively spraining
- History of an ankle sprain weeks to months earlier
- In flatfoot patients: the pain often correlates with arch collapse over the day
A revealing exam test: palpation of the sinus tarsi reproduces the pain exactly, and forced inversion of the hindfoot worsens it.
Diagnosis
Sinus tarsi syndrome is largely a clinical diagnosis — there’s no single test that confirms it. The workup typically includes:
- History and exam — pinpoint tenderness in the sinus tarsi, often with a positive inversion stress test
- Weight-bearing X-rays — to assess hindfoot alignment, rule out fractures and arthritis, and evaluate for flatfoot
- MRI — the most useful imaging test. Shows fluid in the sinus tarsi, ligament tearing, fat replacement, and rules out other causes (talar OCD lesions, occult fractures, peroneal tendon tears)
- Diagnostic injection — placing a small amount of local anesthetic into the sinus tarsi. Pain relief that lasts a few hours strongly supports the diagnosis and is one of the most useful tests when the picture is unclear
Treatment
Conservative care (first-line, usually effective)
- Rest and activity modification — avoid running on uneven surfaces during flares
- NSAIDs for inflammation
- Bracing — a lace-up ankle brace or stirrup-type brace during activity reduces inversion stress
- Custom orthotics — especially important for flatfoot patients. A medial post supports the arch and “opens” the sinus tarsi
- Physical therapy — peroneal strengthening, balance and proprioception work, calf stretching
- Cortisone injection into the sinus tarsi — both diagnostic and therapeutic, and often gives lasting relief in this specific condition
Most patients with isolated sinus tarsi syndrome (without associated structural problems) improve substantially with conservative measures over 6–12 weeks.
When conservative care fails
- Treat the underlying problem first — sinus tarsi syndrome often coexists with chronic ankle instability or progressing flatfoot. Surgery for those root causes (ligament reconstruction, flatfoot correction) often eliminates the sinus tarsi pain
- Sinus tarsi debridement — open or arthroscopic removal of inflamed tissue. Reserved for refractory cases after thorough workup
- Subtalar arthroereisis — placement of a small implant in the sinus tarsi that limits abnormal subtalar motion. Sometimes used in flatfoot reconstruction
Bottom line
Sinus tarsi syndrome is the classic “lingering ankle sprain” — pain in a very specific spot on the outside of the foot that should have resolved but didn’t. It’s also a common driver of pain in adult-acquired flatfoot. The diagnosis is clinical, supported by MRI and confirmed by a diagnostic injection. Conservative care, especially orthotics in flatfoot patients, fixes the majority of cases. If pain persists, the real question is usually whether there’s an underlying instability or flatfoot problem that needs addressing.
Last updated: April 27, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 27, 2026