Quick answer
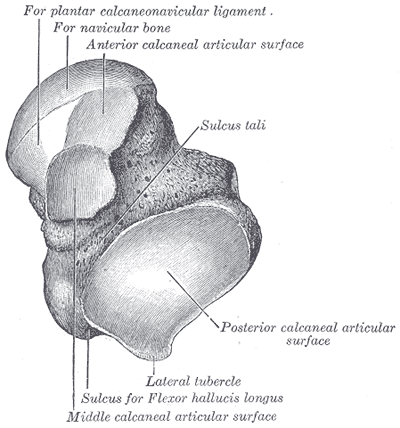
An osteochondral lesion of the talus (OLT) is a damaged area of cartilage and the underlying bone on the talar dome — the dome-shaped top of the talus that articulates with the tibia and fibula. The lesion can range from softened cartilage to a fragment of bone-and-cartilage that has detached and floats in the joint. The most common cause is an ankle sprain in which the talus shears against the malleolus.
How to recognize it
Many OLTs are missed initially because plain X-rays can be normal. The clues come from the pattern of symptoms:
- Persistent ankle pain weeks to months after a sprain that “should” have healed
- Deep aching rather than the surface pain of ligament injury
- Pain with weight bearing, especially on uneven ground
- Recurrent swelling in the ankle
- Catching, locking, or clicking if a fragment is loose
- Stiffness in the morning or after rest
- Pinpoint tenderness on the front-medial or front-lateral corner of the talar dome
Why this happens
The most common mechanism: an ankle sprain in which the talus pinches or shears against the malleolus, damaging a small area of cartilage and the bone just beneath it.
- Lateral lesions (outside corner of the talar dome) typically come from inversion injuries with dorsiflexion
- Medial lesions (inside corner, more common) often come from inversion with plantar flexion
- Atraumatic lesions are sometimes idiopathic — possibly from a vascular insult to a small area of bone (true osteochondritis dissecans)
Regardless of mechanism, the cartilage cap is damaged and the underlying bone often develops a cyst or fragments.
The staging system
Lesions are classified by severity:
- Stage I — softening of the cartilage with intact surface
- Stage II — partial-thickness cartilage tear
- Stage III — non-displaced fragment (cartilage detached but in place)
- Stage IV — displaced fragment (loose body in the joint)
- Stage V — subchondral cyst formation
Stable lesions (Stages I–II) often respond to conservative care. Unstable lesions (Stages III–IV) typically require surgery.
Diagnosis
- Physical exam — tenderness in the joint, swelling, pain with extreme dorsiflexion or plantar flexion
- X-rays — may show the lesion if large or if there’s a loose body, but commonly normal
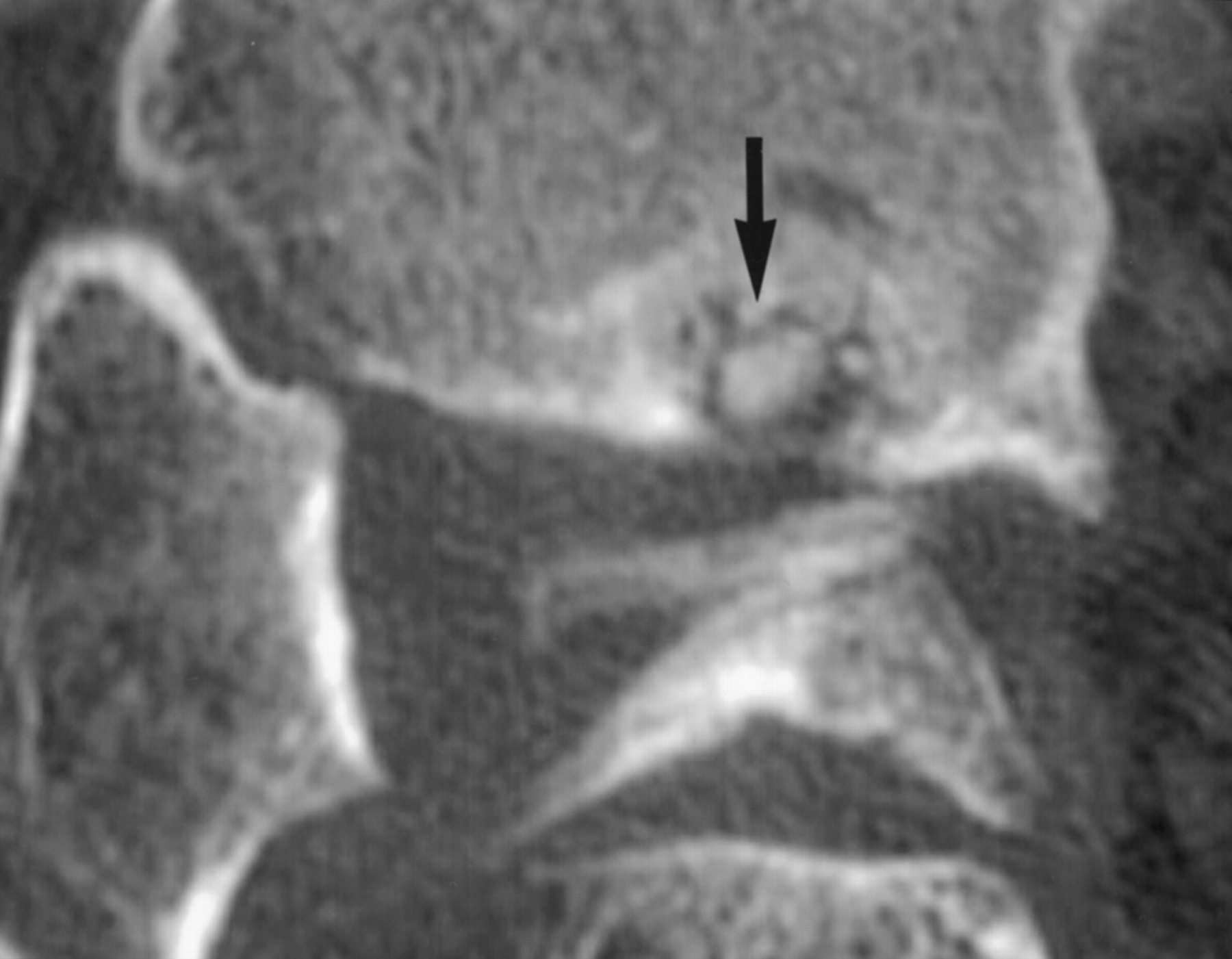
- MRI — gold standard. Shows the cartilage, underlying bone edema, cysts, and any loose fragments
- CT scan — useful for assessing the bony component, especially before surgery
A high index of suspicion is essential: any ankle pain that persists 6 weeks past a sprain deserves an MRI.
Treatment
Conservative care (first-line for stable lesions)
- Activity modification — reduce impact loading
- Walking boot for 6–12 weeks for symptomatic lesions
- Physical therapy — focus on calf flexibility, intrinsic foot strength, and ankle proprioception
- NSAIDs for pain
- Ankle brace during return to activity
- Address the cause — chronic ankle instability needs separate treatment
Conservative care succeeds in roughly 50% of stable lesions. Larger and unstable lesions usually need surgery.
Surgery
For lesions that fail conservative care or are unstable from the start:
- Microfracture — small holes drilled into the bone beneath the lesion to stimulate fibrocartilage formation. Standard for smaller lesions (<1.5 cm²). Good short-term results, but the replacement tissue isn’t true cartilage.
- OATS (osteochondral autograft transfer) — a plug of bone-and-cartilage is harvested from the knee and transferred to the talus. Better long-term durability for larger lesions.
- Allograft transplantation — donor osteochondral plug. Used for very large lesions.
- BMAC (bone marrow aspirate concentrate) and scaffolds — biologic augmentation, increasingly common as adjuncts.
- Loose body removal — for floating fragments causing locking.
Recovery is 3–6 months depending on procedure.
Newer biologic options
- Cartilage cell-based therapies (MACI and similar) — growing patient cartilage cells in a lab and transplanting them. Available for select lesions.
- PRP and bone marrow injections — adjuncts being studied for early-stage lesions.
Bottom line
If an ankle sprain isn’t getting better after 6 weeks, especially with deep aching pain or a catching sensation, an OLT should be considered. Plain X-rays can miss these — MRI is what makes the diagnosis. Stable lesions often respond to rest and rehab; unstable lesions usually need surgery, with several reasonable options depending on lesion size and location.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026