Quick answer
PTTD is when the posterior tibial tendon — a key support of your arch — weakens, stretches, or tears. The arch collapses, the foot rolls inward, and the heel angles outward. Untreated, it’s progressive and can lead to a rigidly flat, painful foot. The good news: caught early, it can usually be managed without surgery.
What this tendon does
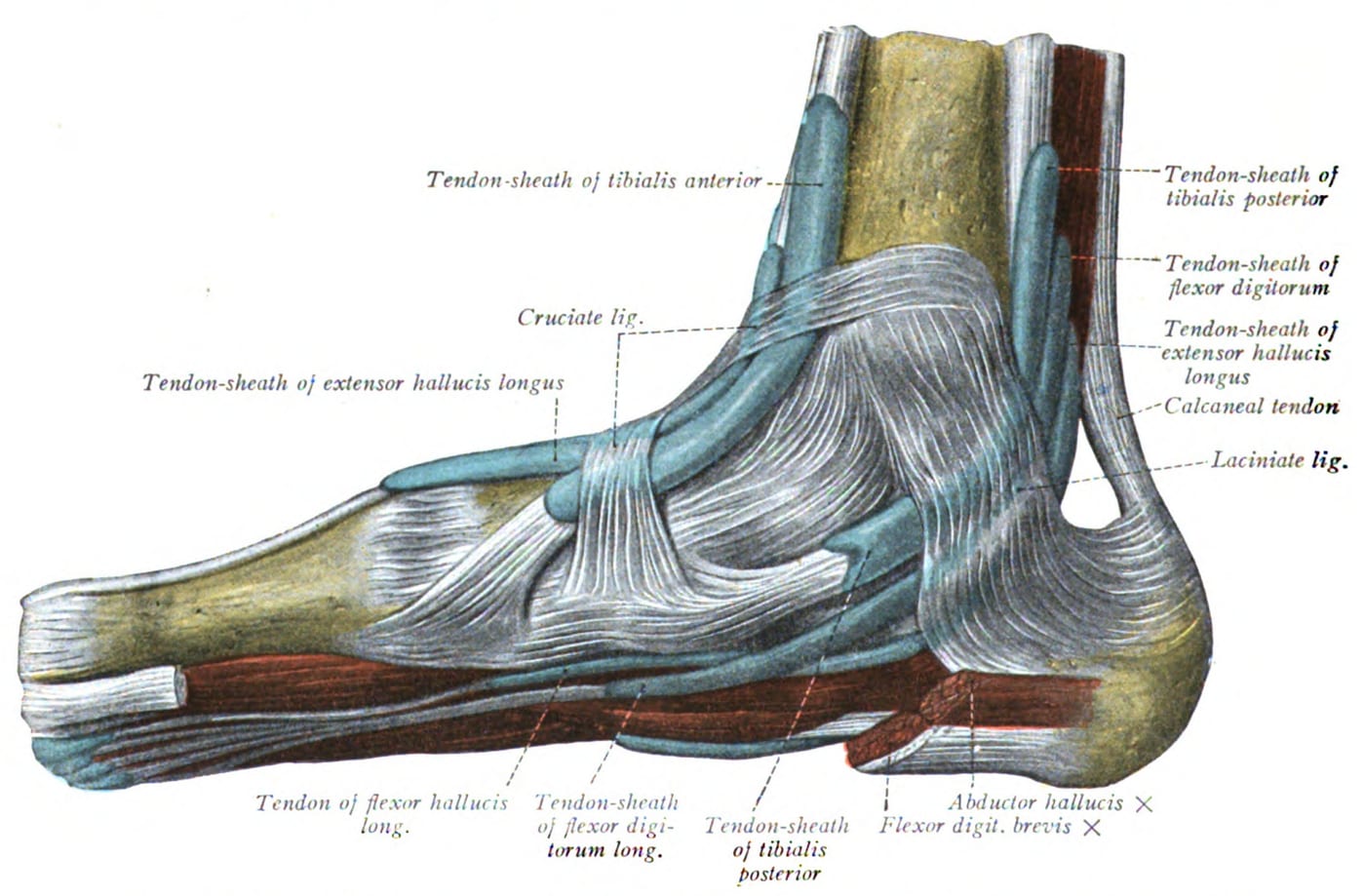
The posterior tibial tendon runs from the calf, behind the inner ankle bone (medial malleolus), and inserts under the arch. Its job:
- Supports the arch during walking
- Locks the midfoot during push-off, so the foot becomes a rigid lever
- Inverts the foot (turns the sole inward)
- Stabilizes the heel against valgus (rolling outward) forces
When this tendon fails, the arch collapses, the heel rolls outward, and the forefoot drifts outward — the classic adult-acquired flatfoot.
How to recognize it
Early signs:
- Pain along the inside of the ankle and arch, especially after activity
- Swelling along the inside of the ankle
- Tired, aching feet at the end of the day
- Difficulty standing on one leg’s tiptoes — the affected side can’t lift the heel as well
- Symptoms worse with prolonged walking or standing
Later signs:
- Visibly flat foot with the arch collapsed
- Heel angled outward when viewed from behind
- “Too many toes” sign — viewing from behind, more toes are visible on the affected side
- Pain shifts to the outside of the ankle as bone-on-bone contact develops, sometimes with sinus tarsi syndrome
- Stiff, rigid flat foot in advanced disease
Stages
PTTD progresses through stages — the staging matters because treatment differs:
- Stage 1 — Tendon inflammation, no deformity yet. Best chance for full recovery.
- Stage 2 — Tendon dysfunction with flexible flat foot. The foot can be passively corrected.
- Stage 3 — Rigid flat foot with arthritis in the hindfoot.
- Stage 4 — Stage 3 plus ankle joint involvement.
The earlier the stage, the more conservative the treatment and the better the outcome.
Why it happens
Risk factors:
- Age — most common in 40s–60s
- Female — significantly more common
- Hypertension
- Diabetes
- Obesity
- Prior ankle injury
- Inflammatory arthritis (rheumatoid)
- Repeated steroid injections in the area
- Genetic predisposition to flat feet
The tendon weakens over time from chronic overload — sometimes accelerated by a specific event but more often gradually.
Treatment
Stage 1 (early)
- Rest — reduce aggravating activity
- NSAIDs for pain
- Ice after activity
- Ankle brace or orthotic to support the arch
- Physical therapy — eccentric strengthening of the tendon
- Calf stretching
Stage 2 (most common stage at presentation)
- Custom orthotics with strong arch support and medial heel posting
- Ankle-foot orthosis (AFO) — for moderate cases; supports the arch and ankle
- Physical therapy — strengthening, stretching, gait training
- Activity modification — limit high-impact, prolonged standing
- Walking boot for acute flares
If conservative care fails after 3–6 months, surgical reconstruction is considered. Procedures vary — typically include tendon transfer (using flexor digitorum longus to replace the failing PTT), calcaneal osteotomy (cutting and shifting the heel bone medially), and other steps to reconstruct the arch.
Stage 3–4 (rigid)
- Bracing for those who can’t have surgery
- Surgical fusion of one or more hindfoot joints (subtalar, talonavicular, calcaneocuboid)
- Triple arthrodesis — fusing all three hindfoot joints; salvage option for severe cases
- Total ankle replacement for stage 4 ankle involvement (selected patients)
When to see a clinician
- Pain on the inside of the ankle that doesn’t resolve in 2–3 weeks
- An arch that’s getting flatter
- Foot that’s rolling inward visibly
- Difficulty rising on one leg’s tiptoes
- “Too many toes” sign noticed by you or others
- You have risk factors (women 40+, diabetes, hypertension, obesity) and any new arch pain
Earlier diagnosis means more options and better outcomes. Stage 1 PTTD is much easier to treat than stage 3.
Prevention
PTTD isn’t fully preventable, but you can lower the risk:
- Manage weight, blood pressure, and diabetes
- Strengthen the calves and feet — heel raises, single-leg balance
- Don’t ignore mild arch or inside-ankle pain — early intervention prevents progression
- Address ankle injuries promptly with proper rehab
- Quality, supportive shoes — especially as you get older
- Custom orthotics if you have flat feet that have started to hurt
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026