Quick answer
In someone with diabetes, a wound that would heal in a week for someone else can take months — long enough for infection to take hold and spread. The combination of reduced sensation, reduced blood flow, and impaired immunity turns minor injuries into serious problems. Early recognition and prompt care prevent most amputations.
Why diabetes makes wounds heal so slowly
Three diabetes-related changes work against healing:
1. Reduced sensation
Diabetic neuropathy means a wound or pressure point isn’t felt. The patient keeps walking on the area, preventing healing. A simple blister gets stepped on a thousand more times.
2. Reduced blood flow
Peripheral arterial disease — narrowed arteries — reduces oxygen and nutrient delivery to the foot. Healing requires both. The same wound that has plenty of blood flow heals quickly elsewhere; in a diabetic foot with PAD it can be stalled indefinitely.
3. Impaired immune response
High blood glucose affects neutrophil function — the immune cells that fight bacterial infections. Bacteria that would be cleared in a non-diabetic wound establish a foothold and multiply.
Add biomechanical changes (concentrated pressure points), glycation (stiffened tissue), and autonomic dysfunction (impaired sweating, drier skin), and the cascade is set up.
What every diabetic wound needs to heal
No matter how complicated the case, every diabetic foot wound needs three things to heal. If any one is missing, the wound stalls — and most cases that fail to heal come down to one or more of these being neglected.
1. Offloading — taking pressure off the wound
A wound that’s being walked on can’t heal. Repeated pressure tears apart fragile new tissue with every step, and a plantar ulcer that takes weight all day will look the same in three months as it did the day it appeared. Common offloading methods:
- Total contact cast (TCC) — gold standard for plantar ulcers; redistributes weight across the entire lower leg
- Removable cast walker (CAM boot) — when a TCC isn’t tolerated, but only works if the patient actually keeps it on
- Custom offloading shoes with relief cutouts over the wound area
- Crutches, knee scooter, or wheelchair for severe cases or non-plantar wounds
- Felt padding and accommodative inserts for less severe wounds
The wound has to be offloaded 24/7, not just outside the house. A patient who walks barefoot to the bathroom at night undoes a week of healing.
2. Infection control — eliminating bacteria
If there’s an active infection, the wound won’t heal until it’s controlled — and a wound that looks “stuck” is often quietly infected. Infection control means:
- Recognizing it early — see warning signs below
- Appropriate antibiotics — guided by wound culture when possible, empiric when not
- Surgical debridement of dead and infected tissue — often the single most important step in moderate-to-severe cases
- Treating any underlying osteomyelitis — bone infection won’t clear with topical care alone
3. Adequate blood supply — getting oxygen to the wound
Healing is metabolically expensive; it requires oxygen and nutrients delivered through arteries. If the arteries are blocked — peripheral arterial disease, very common in long-standing diabetes — no amount of dressing changes or antibiotics will close the wound. Every non-healing diabetic foot wound deserves a vascular evaluation:
- Pulse exam — basic but essential first check
- Ankle-brachial index (ABI) or toe pressures to quantify flow
- Arterial Doppler ultrasound to map where the blockages are
- Vascular surgery referral when flow is inadequate
- Revascularization — angioplasty, stent, or bypass to restore flow. After successful revascularization, wounds that wouldn’t heal for months often close in weeks.
A wound that isn’t healing despite good wound care is almost always failing for one of these three reasons. Identifying which — or which combination — is what gets it to close.
Warning signs of infection
A wound that’s just slow-healing is one thing. A wound that’s becoming infected needs urgent attention. Signs to watch for:
Local signs
- Increasing redness spreading beyond the wound edge
- Increased warmth of the surrounding skin
- Increased swelling
- Drainage — especially if cloudy, purulent, or smells foul
- Increased pain (though this may be absent if neuropathy is severe)
- Wound expansion — getting larger or deeper
- Visible bone or tendon in the wound base
- Crepitus — a crackling under the skin (a sign of gas-producing bacteria — emergency)
Systemic signs
- Fever
- Chills
- Elevated heart rate
- Confusion (especially in older adults)
- Worsened glucose control — high sugars often accompany infection
Any of these warrants same-day evaluation, not waiting until tomorrow or the next clinic appointment. Diabetic foot infections can progress rapidly to limb-threatening conditions.
Severity grading
Diabetic foot infections are typically classified as:
- Mild — limited to skin and immediate underlying tissue, no systemic signs
- Moderate — extends deeper or wider; possibly into muscle, joint, or tendon; no systemic toxicity
- Severe — systemic signs (fever, low blood pressure, elevated heart rate) — sepsis territory
- Osteomyelitis — infection has reached bone
Severity drives treatment intensity (oral vs IV antibiotics, outpatient vs hospital, surgery vs medical management).
When it becomes life-threatening: necrotizing fasciitis
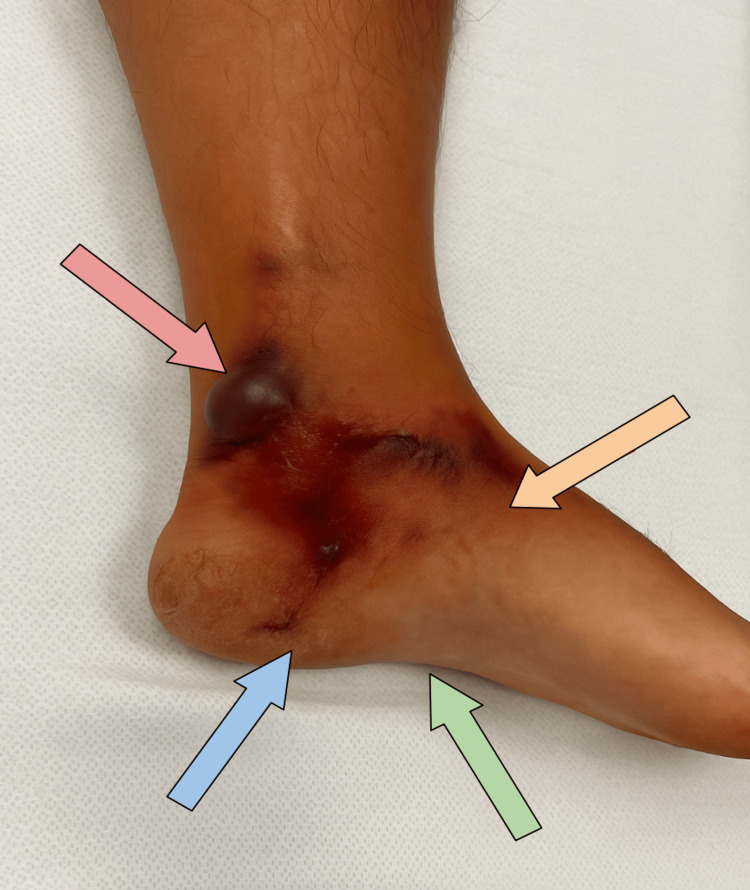
A small fraction of soft-tissue infections become necrotizing fasciitis — a rapidly spreading infection that destroys the deeper fascia and surrounding tissue. Necrotizing fasciitis can progress in hours, not days, and carries a real mortality risk even with the most aggressive treatment.
In a diabetic foot, necrotizing fasciitis most often starts as an unrecognized or undertreated soft-tissue infection — a small ulcer, an infected blister, or a self-drained abscess — and tracks rapidly along the fascial planes between muscle and skin.
Signs that suggest necrotizing fasciitis, not ordinary cellulitis
- Pain disproportionate to what’s visible on the surface
- Skin discoloration — dusky red, purple, or black patches
- Hemorrhagic blisters or bullae (blood-filled blisters)
- Crepitus — a crackling sensation when the skin is pressed, from gas in the tissue
- Rapid spread — measurable progression hour to hour, not day to day
- Systemic toxicity — high fever, low blood pressure, fast heart rate, confusion
Necrotizing fasciitis is a surgical emergency. The only effective treatment is immediate, aggressive surgical debridement — removing all dead and infected tissue, even if that means losing significant amounts of skin, muscle, or limb. Antibiotics alone do not cure it.
Click to show clinical photo: necrotizing fasciitis at presentation (graphic)
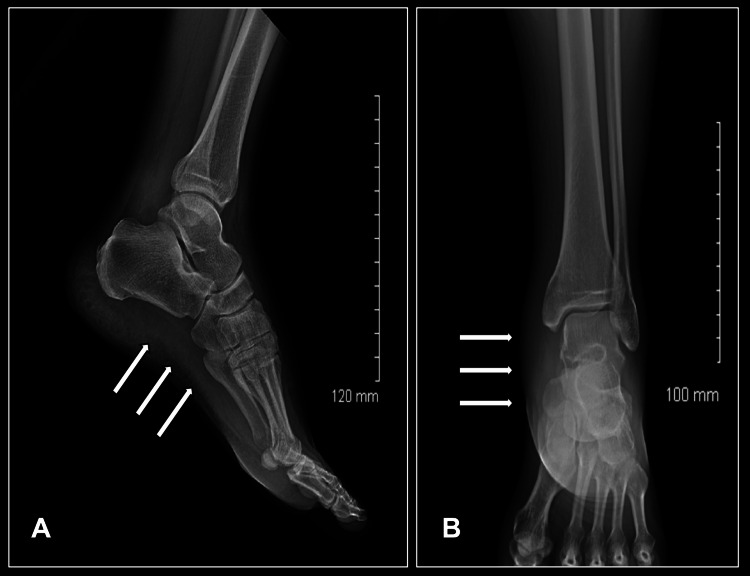
Click to show X-ray: gas in the soft tissues
Click to show surgical photo: extensive debridement (very graphic)
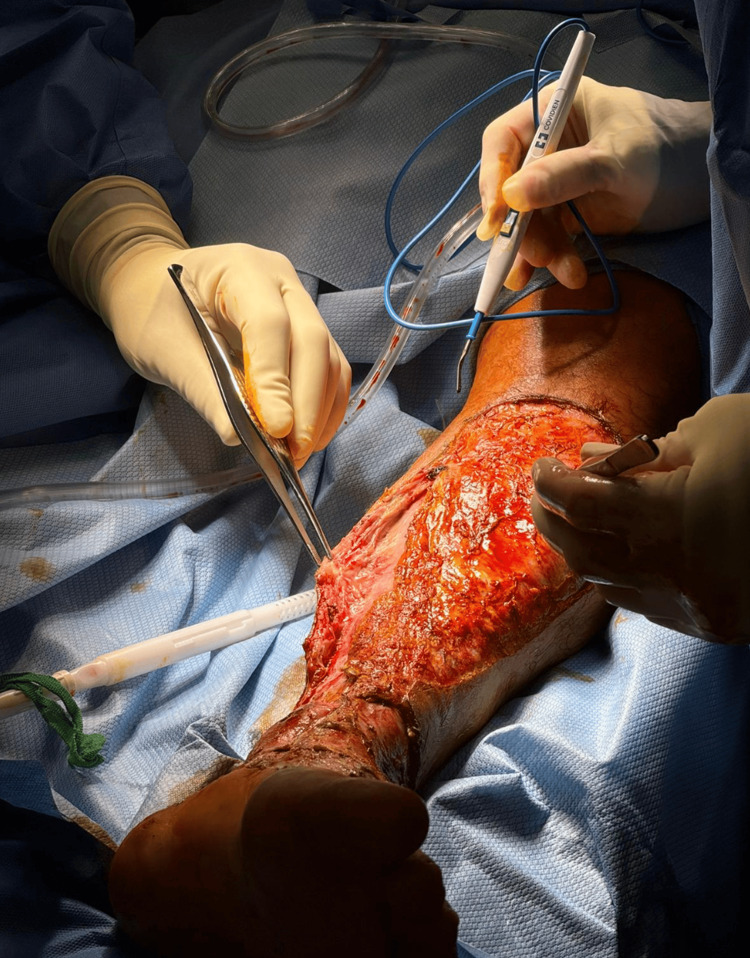
The case shown above (a 52-year-old man who developed necrotizing fasciitis after self-draining an abscess with an unsterilized safety pin) survived because of prompt recognition and aggressive surgical care. Time matters: every hour of delay increases tissue loss and mortality. The same urgency applies in diabetic feet, where blunted pain perception can delay both the patient’s recognition and the clinician’s diagnosis.
Treatment
Mild infections
- Oral antibiotics — typically covering staph and strep
- Wound care — debridement, appropriate dressings
- Offloading — keeping pressure off the wound
- Close follow-up — every 2–7 days initially
Moderate infections
- Often start with IV antibiotics in clinic or short hospital stay
- Broader-spectrum antibiotics — covering more bacterial types
- Debridement — sometimes surgical
- Hospitalization for some
Severe infections
- Hospital admission
- IV broad-spectrum antibiotics
- Urgent surgical evaluation — may need debridement or amputation of necrotic tissue
- Blood cultures, supportive care
- Multidisciplinary team — infectious disease, vascular surgery, podiatry, internal medicine
Osteomyelitis (bone infection)
- Prolonged antibiotic therapy (typically 6+ weeks)
- Often surgical debridement of infected bone
- MRI to guide extent
- Long, complex care often coordinated by a multidisciplinary team
Vascular evaluation
If healing is slow and arterial disease is suspected:
- Ankle-brachial index to screen
- Vascular consultation
- Revascularization (angioplasty, bypass) when indicated — restores blood flow needed for healing
When to see a clinician
Same day:
- Any new foot wound, even if it seems minor
- Blister, especially if filled with cloudy fluid
- Color change in any area of the foot — red, blue, black
- Increasing warmth in one part of the foot
- Wound that’s growing or draining
- Fever in someone with a foot wound
- Streaks of red traveling up the leg
- Any concern at all — better safe than sorry
Don’t wait until your next routine appointment. The 24–48 hours after warning signs first appear is often the difference between an outpatient course of antibiotics and a hospitalization with surgical debridement.
Real-case example: a puncture wound that became osteomyelitis
A published case report in Cureus (2026) illustrates how a seemingly minor wound in a diabetic patient can progress to limb-threatening infection.
A 62-year-old woman with uncontrolled type 2 diabetes stepped on a nail that went through her shoe. She was treated as outpatient cellulitis with oral cephalexin, but the infection didn’t respond. Within days, X-rays revealed MRSA osteomyelitis of the 5th metatarsal — the bone was being eaten away. The case ultimately required IV antibiotics and a ray amputation (surgical removal of the 5th toe along with its metatarsal). She recovered.
The lesson maps directly to the three healing pillars described earlier. Infection control required IV — not oral — antibiotics, plus surgical debridement. Offloading had to be enforced post-op for healing. And the underlying diabetic state (uncontrolled glucose, blunted immune response) worked against every step. Early aggressive imaging (X-rays at first visit, not after antibiotics fail) and a low threshold for IV therapy can change the outcome.
Click to show clinical photo: the wound at presentation (graphic)

Click to show X-ray: bone destruction (osteomyelitis)

Click to show post-amputation photo (very graphic)

Prevention
The most effective prevention is the same as for diabetic foot ulcers in general:
- Daily foot inspection — top, bottom, between toes
- Don’t go barefoot — even at home
- Properly fitted shoes at all times
- Check inside shoes before putting them on
- Treat dry skin and cracks preventively
- Clip toenails straight across; get them done by a professional if you have neuropathy
- Address minor problems early — calluses, blisters, ingrown nails — before they break the skin
- Tight glucose control — better for healing AND for slowing the underlying changes
- Don’t smoke — dramatically worsens both arterial disease and healing
- Annual or more frequent foot exams by a clinician
Bottom line
In diabetes, time is tissue. A foot wound that gets evaluated and treated in 24–48 hours of appearing has a much better outcome than one ignored for a week. The pattern of “I figured it would heal” leading to a serious infection is depressingly common — and almost always preventable with prompt action.
Sources
- Salib M, Salib J, Hildenbrandt EA, Hoffman ME, Tiesenga F. Rapidly Progressive Necrotizing Fasciitis of the Lower Limb Following Self-Drainage of an Abscess. Cureus. 2025. (CC BY 4.0) ↗
- Juybari C, Beeson D, Samones E, Allison RM. X-ray Findings in a Case of Acute Osteomyelitis Following Puncture Injury: A Case Report. Cureus. 2026. (CC BY 4.0) ↗
Last updated: April 30, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 30, 2026