
Quick answer
The cuboid is a small, roughly cube-shaped bone on the outer (lateral) side of the midfoot, sitting between the calcaneus (heel bone) and the 4th and 5th metatarsals. Fractures here are often dismissed as a bad sprain — they’re frequently subtle on initial X-rays and easily overlooked. Most isolated cuboid fractures heal well with immobilization, but the severe “nutcracker” variant involves significant compression and often requires surgery.
A fracture is not the only way the cuboid causes lateral midfoot pain. Cuboid syndrome — a partial dislocation (subluxation) of the bone, especially after lateral ankle sprains — produces a similar pain pattern with completely normal X-rays. The two can look alike on history alone but separate clearly on imaging.
Fracture types
Avulsion fracture — the most common type. A ligament or the peroneus longus tendon pulls off a small flake of bone during a lateral ankle sprain or inversion injury. Often subtle on X-ray. Treated like a sprain, with a boot.
Nutcracker fracture (compression fracture) — a higher-energy injury caused by forced abduction (outward twisting) of the forefoot against a fixed heel. The cuboid is literally crushed between the calcaneus and the 4th/5th metatarsal bases. This can occur in equestrian falls, car accidents, or falls from height. Associated with Lisfranc-type injury patterns.
Stress fracture — gradual onset in runners, dancers, and military recruits from repetitive loading. X-rays initially normal; MRI or bone scan confirms diagnosis.
The “missed” fracture problem
Cuboid fractures are one of the more commonly missed fractures in the foot. The reasons:
- Subtle X-ray findings: Small avulsion chips are easy to overlook, and non-displaced compression fractures may not be obvious on standard views.
- Mimics a sprain: The mechanism (ankle roll, lateral foot injury) is identical to an ankle sprain.
- Patient presentation: Patients often bear weight — at least partially — which creates a false impression that the injury is minor.
If a patient has mid-lateral foot pain, point tenderness over the cuboid, and significant swelling after an ankle-type injury, cuboid fracture must be considered even if initial X-rays look normal.
How to recognize one
Classic history: A twisting fall where the foot rolled inward (inversion injury), a midfoot crush injury, or gradually worsening outer midfoot pain with activity.
Symptoms:
- Pain and tenderness specifically over the outer midfoot (the bump you can feel just below and in front of the lateral ankle)
- Swelling and bruising on the outer foot and ankle
- Pain with weight-bearing; some patients can limp-walk, others cannot bear weight at all
- Pain with toe push-off (the peroneus longus tendon runs in a groove along the cuboid)
How it is diagnosed
X-ray: Three standard views of the foot (AP, lateral, oblique). Many cuboid fractures are visible on careful review. The oblique view is most helpful. Small avulsion flakes may be subtle.
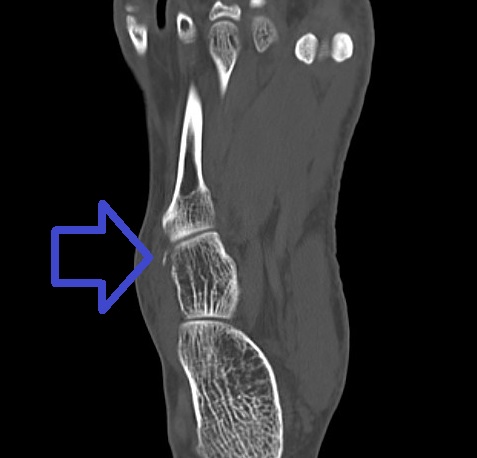
CT scan: Best for confirming the fracture and assessing compression. Essential for nutcracker fractures to determine the degree of comminution and whether the 4th/5th metatarsal articulations are involved.
MRI: Best for stress fractures and for evaluating soft tissue injury (peroneus longus tendon, ligaments) when the diagnosis is uncertain.
Treatment
Non-surgical (most cuboid fractures)
Avulsion fractures and non-displaced fractures:
- Walking boot or short leg cast for 4–6 weeks
- Progressive weight-bearing as tolerated
- Transition to supportive shoes; lateral heel wedge if peroneus longus tendon irritation persists
Stress fractures:
- Activity modification; boot or NWB depending on severity
- Address the underlying training load or nutritional factors
Surgical (nutcracker fractures and displaced fractures)
Significant compression of the cuboid with collapse of the lateral column of the foot typically requires surgery:
External fixation or ORIF: The lateral column is restored to its correct length (distraction). Bone graft is often used to fill the crushed defect. Plates and screws maintain alignment.
Goal: Restore the length and alignment of the lateral column. Loss of length here causes the foot to collapse outward (planus deformity) and disrupts the mechanics of the 4th and 5th metatarsals.
Recovery
| Fracture type | Boot/NWB | Return to activity |
|---|---|---|
| Avulsion fracture | 4–6 weeks | 8–10 weeks |
| Stress fracture | 6–8 weeks | 10–14 weeks |
| Nutcracker (non-surgical) | 8–10 weeks | 4–6 months |
| Nutcracker (surgical) | 10–12 weeks | 5–8 months |
Long-term stiffness in the subtalar and midtarsal joints is common after significant cuboid fractures. A lateral wedge or custom orthotic often helps manage persistent discomfort.
Don’t miss the Lisfranc connection
Cuboid fractures — especially nutcracker patterns — frequently occur alongside Lisfranc (tarsometatarsal joint) injuries. If there’s any midfoot tenderness, swelling across the dorsum of the foot, or bruising at the base of the 2nd toe (plantar ecchymosis), Lisfranc injury must be evaluated with weight-bearing X-rays.
The main thing to understand
Most cuboid fractures look like bad ankle sprains, and that’s exactly why they get missed. If the tenderness is over the lateral midfoot (not the lateral ankle), and the swelling is significant, imaging of the foot — not just the ankle — is warranted. The avulsion type heals well with a boot. The nutcracker type is a different beast that needs specialist evaluation.
Last updated: April 26, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 26, 2026