Quick answer
Tarsal tunnel syndrome is compression of the posterior tibial nerve as it passes through a narrow space behind the inner ankle bone (the tarsal tunnel). Like carpal tunnel in the wrist, it produces burning, tingling, and sometimes shooting pain — in this case in the inner ankle, arch, or toes. The diagnosis is often missed because it’s less common than other foot conditions, but it has effective treatments when recognized.
How to recognize it
Symptoms often described:
- Burning in the inner ankle, arch, or sole
- Tingling (“pins and needles”) in the same areas
- Electric shocks radiating into the toes
- Numbness in parts of the sole
- Worse with standing, walking, or activity
- Sometimes worse at night in bed
- A “feeling of fullness” in the ankle
- Symptoms reproduced by tapping behind the inner ankle (Tinel’s sign)
The pattern matters. Pain in the foot’s BOTTOM (sole) coming from a problem at the inside of the ANKLE is the signature of TTS.
Why it happens
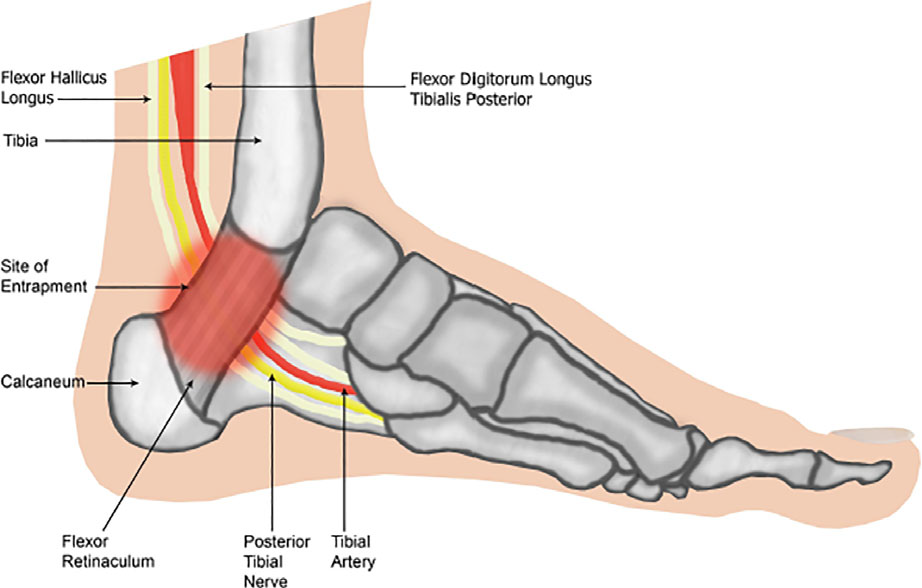
The tarsal tunnel is a fibrous passageway behind the inner ankle bone. The posterior tibial nerve, plus an artery, vein, and several tendons, all pass through. Anything that crowds this space can compress the nerve:
- Flat feet — the chronically stretched nerve is at higher risk
- Ankle injuries — sprains, fractures cause swelling that compresses the nerve
- Varicose veins in the area
- Ganglion cysts
- Bone spurs
- Tumors (rare)
- Tenosynovitis (inflammation of the surrounding tendon sheaths)
- Systemic conditions — diabetes, hypothyroidism, rheumatoid arthritis (chronic swelling)
- Pregnancy — fluid retention
- Repeated impact activities — running, dancing on hard surfaces
About half of cases have an identifiable cause (a “space-occupying lesion”). The rest are “idiopathic” — no specific structural cause found.
Diagnosis
Clinical exam is the starting point:
- Tinel’s sign — tapping behind the inner ankle reproduces the symptoms
- Provocative testing — holding the foot in eversion and dorsiflexion can reproduce pain
- Sensation testing in the foot
Imaging and nerve studies often follow:
- MRI — looks for ganglion cysts, varicose veins, tumors, or other space-occupying lesions
- Ultrasound — alternative for visualizing soft tissue
- Nerve conduction studies / EMG — confirms nerve compression and can help differentiate from other neuropathies (though normal results don’t rule out TTS)
- X-rays — for bone spurs or coalitions
Treatment
Conservative care (first-line for most cases)
- Custom orthotics — supporting the arch reduces tension on the nerve. Often the single most helpful intervention for TTS associated with flat feet.
- NSAIDs — for inflammation and pain
- Physical therapy — stretching, nerve glides, calf flexibility
- Activity modification — temporarily reduce high-impact activities
- Ice for acute flares
- Bracing for severe cases — ankle stabilization
- Steroid injection into the tarsal tunnel — can reduce inflammation around the nerve; provides diagnostic information too
Surgery (for cases that fail conservative care)
Tarsal tunnel release — opens the fibrous roof of the tunnel and decompresses the nerve. Outcomes:
- Best for cases with identifiable structural causes (ganglion, varicosity, etc.)
- Mixed for idiopathic TTS — symptom improvement varies widely
- Recovery typically 6–8 weeks
- Complete relief in 50–80% depending on the underlying cause
This is one of those conditions where careful patient selection for surgery matters a lot. Idiopathic TTS without a clear lesion has worse surgical outcomes than TTS with an obvious cause.
When to see a clinician
- Burning or tingling in the inner ankle, arch, or sole
- Symptoms persisting more than 2 weeks
- Symptoms worsening with activity
- Numbness or weakness in the foot
- Recent injury followed by these symptoms
- History of flat feet plus new burning/tingling
- Symptoms that wake you at night
A foot specialist (podiatrist or orthopedic surgeon) is the right starting point. They can:
- Confirm the diagnosis
- Order appropriate imaging
- Distinguish TTS from other causes of similar symptoms
- Recommend conservative management
Look-alikes worth considering
Several conditions can mimic tarsal tunnel:
- Plantar fasciitis — heel pain rather than burning/tingling
- Diabetic neuropathy — usually bilateral (both feet), starts at the toes
- Lumbar radiculopathy (pinched nerve in the back) — pain can radiate down the leg into the foot
- Morton’s neuroma — burning specifically between the toes (forefoot, not inner ankle)
- Charcot-Marie-Tooth disease — inherited neuropathy, broader symptoms
A careful exam and sometimes imaging or nerve studies sort these out.
Prevention
- Address flat feet with orthotics if you have arch pain
- Proper rehab after ankle injuries to limit chronic swelling
- Manage systemic conditions — diabetes, hypothyroidism, RA — that contribute
- Quality footwear with adequate arch support
- Don’t ignore early symptoms — early intervention is more reliable than treating chronic TTS
Frequently asked questions
What is tarsal tunnel syndrome?
Tarsal tunnel syndrome is compression of the posterior tibial nerve (and its branches) as it passes through the tarsal tunnel — a narrow space behind the inner ankle bone (medial malleolus), bounded above by a tough fascial ligament (the flexor retinaculum). It's often described as the foot's version of carpal tunnel syndrome. Compression in this small space produces burning, tingling, electric, or shooting pain in the inner ankle, arch, heel, or toes — depending on which branches of the nerve are most affected.
What does tarsal tunnel syndrome feel like?
Most patients describe one or more of: burning pain on the inside of the ankle that radiates down into the arch or toes, tingling or 'pins and needles' in the bottom of the foot, electric or shooting pain with certain ankle positions, numbness in part of the sole, and worse symptoms at night or after prolonged standing. The pain typically worsens with activity and may briefly improve with rest. The Tinel's sign (tapping over the inner ankle reproduces the tingling shock down into the foot) is the classic exam finding.
How is tarsal tunnel syndrome diagnosed?
Diagnosis is mostly clinical — the combination of typical symptom pattern, a positive Tinel's sign over the tarsal tunnel, and exclusion of mimics (especially plantar fasciitis and Baxter's neuritis). Nerve conduction studies and EMG can confirm the diagnosis and quantify severity, though they're not always positive in mild cases. MRI is useful for finding a specific compressive lesion within the tunnel — a ganglion cyst, varicose vein, accessory muscle, or bone spur — which then guides whether surgery is likely to help.
How is tarsal tunnel syndrome different from plantar fasciitis?
Both cause heel and arch pain, but the patterns differ. Plantar fasciitis classically causes sharp, mechanical pain with the first morning steps that warms up with walking, with point tenderness at the front-center of the heel. Tarsal tunnel syndrome causes burning or tingling nerve pain rather than sharp mechanical pain, often worse at night and with prolonged standing, and may radiate into the toes or arch. Patients often have both, which complicates the picture — the distinguishing test is the Tinel's sign at the inner ankle, which is absent in pure plantar fasciitis.
How is tarsal tunnel syndrome treated?
First-line is conservative: supportive shoes, custom orthotics that correct overpronation and reduce traction on the nerve, calf stretching, activity modification, NSAIDs, and sometimes a corticosteroid injection at the tunnel. If a specific compressive lesion (cyst, bone spur, accessory muscle) is found on MRI, treating that lesion often resolves the symptoms. When conservative care fails after 3 to 6 months, surgical decompression (release of the flexor retinaculum, sometimes with removal of the compressive structure) is the next step. Surgical results are best when an anatomical cause has been identified pre-op.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026