Quick answer
Plantar fasciitis is irritation of the thick band of tissue (the plantar fascia) that runs along the bottom of your foot, connecting the heel bone to the toes. The hallmark sign: sharp, stabbing heel pain with the first steps in the morning, which eases after a few minutes of walking and then returns later in the day.
It’s the most common cause of heel pain in adults, affecting about 1 in 10 people in their lifetime. The good news: roughly 80 to 90% of cases resolve within 6 to 12 months even with minimal treatment, and active treatment (orthotics, daily stretching, physical therapy) often shortens this to 6 to 12 weeks when patients commit to it. Stretching, supportive footwear, and patience remain the cornerstones.
What it is
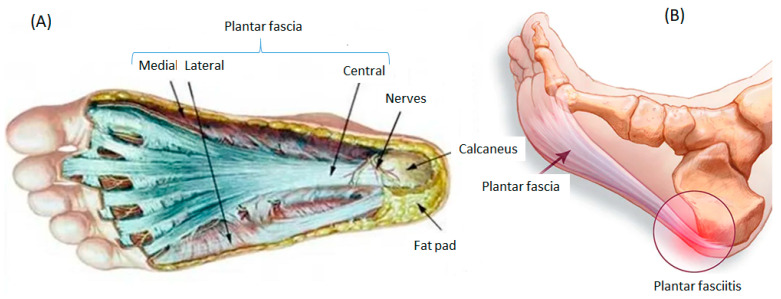
The plantar fascia is a strong, fibrous band of connective tissue that runs from the heel bone (calcaneus) along the bottom of the foot to the base of the toes. It supports the arch, absorbs shock, and stores energy with each step.
Plantar fasciitis is irritation and microscopic tears in this tissue, usually where it attaches to the heel. Despite the “-itis” suffix (which implies inflammation), current research shows it’s more often a degenerative condition (technically called plantar fasciopathy in the research literature) — the tissue becomes disorganized and weakened from repeated stress, with relatively little classical inflammation. The treatment implications are practical: tissue regeneration takes time, which is why recovery measures in months, not weeks. We use “plantar fasciitis” throughout because it remains the term most patients and clinicians recognize.
Why the morning pain pattern is so distinctive
While you sleep, your foot rests in a slightly pointed position (plantarflexion), and the plantar fascia shortens. Healing tissue lays down small adhesions overnight. When you put weight on the foot in the morning, those adhesions tear apart, producing the classic stabbing pain.
After a few minutes of walking, the fascia warms up and elongates, and the pain eases. But sit for an hour and the cycle repeats: the first few steps after sitting hurt again. This post-static dyskinesia pattern is so characteristic that it’s nearly diagnostic on its own.
Symptoms
- Sharp, stabbing pain in the heel with the first steps in the morning or after periods of sitting
- Pain concentrated at the inside-front of the heel (medial calcaneal tubercle)
- Pain that eases with walking for a few minutes, then returns at the end of the day
- Pain after exercise, not usually during
- Worse barefoot or on hard floors
- Better in supportive shoes, especially with arch support
- Often one-sided, but can affect both feet
Two patterns of plantar fasciitis
Acute flare
A discrete period of worsening pain, usually triggered by a specific event: starting a running program, switching to less supportive shoes, sudden weight gain, or pregnancy. Pain comes on over days to weeks. Caught early and treated consistently, often resolves within 2 to 4 months.
Chronic plantar fasciitis
Persistent symptoms lasting more than 6 months despite conservative care. Tissue is disorganized rather than acutely inflamed (the technical term is chronic plantar fasciopathy). Treatment shifts from rest and ice toward active interventions like shockwave therapy, PRP, or surgery. About 10 to 20% of cases become chronic.
What causes it
The plantar fascia is built to handle stress, but accumulated overload causes the tissue to break down faster than it can repair. The most common contributing factors:
- Sudden increase in activity — new running program, switching from desk job to standing job, training mileage jumped too fast
- Foot mechanics — flat feet, high arches, or excessive pronation
- Tight calf muscles — limit ankle dorsiflexion, transferring load onto the fascia. Often the single most underrated driver.
- Age 40 to 60 — peak incidence range
- Higher body weight — every walking step transmits roughly 1.1 to 1.5 times body weight through the heel; running steps transmit 3 to 4 times body weight
- Pregnancy and the postpartum period — weight changes plus relaxin-related ligament laxity
- Worn-out or unsupportive shoes — flat shoes, old running shoes, minimalist footwear without arch support
- Hard surfaces — concrete floors at work, hard treadmills
- Occupations that involve prolonged standing — teachers, nurses, retail workers, factory workers
How it’s different from other heel pain
Heel pain has many causes, and the wrong diagnosis means the wrong treatment. The most common look-alikes:
| Condition | Key distinction from plantar fasciitis |
|---|---|
| Heel spurs | Often coexist with plantar fasciitis; the spur itself is usually painless. The fascia is the source of pain in nearly all cases. |
| Calcaneal stress fracture | Pain is more diffuse across the whole heel, not pinpoint at the medial tubercle. Often tender to side-to-side compression of the heel. Worse with walking, not just first steps. |
| Tarsal tunnel syndrome | Burning or tingling pain rather than sharp; often radiates into the arch or toes. Worse with prolonged standing or at night. |
| Baxter’s neuritis | Burning or radiating pain, tender spot slightly more medial and lower than the classic fasciitis spot, doesn’t have the classic morning-pain warm-up pattern. Accounts for an estimated 15-20% of “treatment-resistant plantar fasciitis.” |
| Plantar fibroma / Ledderhose disease | A firm, fixed lump or lumps within the arch tissue (palpable as a knot in the fascia). Pain pattern is from shoe pressure on the nodule, not the morning-stabbing pattern of fasciitis. |
| Achilles tendinitis | Pain at the back of the heel, not the underside. Pain with calf engagement. |
| Inferior calcaneal bursitis | Pain in the heel pad rather than the medial tubercle. Often follows a fall or hard heel strike. |
| Sever’s disease | Children only (ages 8 to 14). Heel growth plate. |
| Fat pad atrophy | Generalized heel pain, worse with hard surfaces. Heel pad feels thin. More common in older adults. |
If your pain doesn’t fit the morning-stabbing pattern, the diagnosis may not be plantar fasciitis. A podiatrist or sports medicine clinician can usually distinguish them on exam alone.
Treatment options (the stepwise hierarchy)
The goal is to offload the irritated tissue while addressing the mechanical drivers. Try each stage for 4 to 6 weeks before escalating.
Stage 1 — Self-care basics (first 4 to 6 weeks)
- Stretching twice daily. Calf stretches plus the plantar fascia-specific stretch (toes pulled back toward shin). 10 reps, 10 seconds each, 3 sessions per day. Most underrated step.
- Supportive shoes worn all day, including at home. Replace any shoe with worn-down heel cushioning. Look for built-in arch support and a slight heel-to-toe drop (10 to 12 mm).
- Ice rolling. Frozen water bottle under the arch for 10 to 15 minutes after activity or at the end of the day.
- Activity modification. Reduce or stop the activity that triggered the flare (running, long walks). Cross-train with cycling or swimming.
- Avoid barefoot walking on hard floors. Even at home, slip on supportive sandals or shoes.
- Over-the-counter pain control. NSAIDs (ibuprofen, naproxen) for short bursts of acute pain. Not recommended long-term.
Stage 2 — Add supportive devices (weeks 4 to 8)
- Over-the-counter orthotics or heel cups. Look for firm arch support, not just gel cushioning. Brands like Powerstep, Superfeet, and Vionic are commonly recommended.
- Night splints. Sock-style (Strassburg Sock) or rigid boot designs. Hold the foot at 90 degrees overnight to prevent the fascia from tightening. Most effective for chronic morning pain.
- Heel cups inside athletic shoes. Silicone heel cups can absorb shock for runners returning to training.
- Continue stretching. This is the foundation through every stage.
Stage 3 — Clinical interventions (months 3 to 6+)
- Custom orthotics. Prescribed by a podiatrist, made specifically for your foot mechanics. More effective than OTC for biomechanical drivers.
- Physical therapy. Hands-on soft-tissue work, intrinsic foot strengthening, calf eccentric loading. Often dramatically helpful for cases that have plateaued.
- Corticosteroid injection. Real short-term relief; practice on frequency varies. A cautious approach limits to 1 or 2 injections per heel per lifetime; common clinical practice allows up to 3 per year for stubborn cases. Each injection carries cumulative risk of fat pad thinning and fascial rupture.
- Extracorporeal shockwave therapy (ESWT). Non-invasive, uses focused acoustic waves to stimulate healing. Multiple clinic sessions over 4 to 6 weeks. Good evidence for chronic cases.
- Platelet-rich plasma (PRP) injection. Patient’s own concentrated platelets injected into the fascia. Promising for chronic cases that haven’t responded to other treatments. Cost is often out of pocket.
Stage 4 — Surgery (rarely needed)
- Plantar fascia release (either open or endoscopic). The fascia is partially cut to release tension.
- Reserved for cases that have failed 12+ months of consistent conservative and clinical care.
- About 70 to 80% good outcomes, but recovery is months and there’s a small risk of arch collapse if too much fascia is released.
What does NOT work (skip these)
- Sleeping with no shoes and waking up to walk barefoot. Worst possible morning sequence. Put on supportive shoes before standing up.
- Aggressive stretching of an acutely painful fascia. Gentle stretching helps; forceful stretching can tear weakened tissue.
- Long-term NSAIDs. Useful for a flare; not a treatment plan. Chronic NSAID use also delays tissue healing.
- Repeat cortisone injections. Each one weakens the fascia further.
- Buying expensive insoles without addressing tight calves. The single most overlooked cause; no insole fixes equinus.
- Resting completely. Some activity restriction helps; bed rest weakens the foot and prolongs recovery.
Recovery timeline (what to actually expect)
| Stage | Timeline | What to expect |
|---|---|---|
| First month | Weeks 1 to 4 | Mild improvement with consistent self-care. Morning pain still present but slightly less sharp. |
| Months 2 to 3 | Weeks 5 to 12 | Most patients see meaningful improvement: shorter morning pain, longer pain-free walking. Many people start to think they’re cured here, then push too hard and re-flare. |
| Months 4 to 6 | Weeks 13 to 24 | Significant relief for most. Returning gradually to running and high-impact activities. |
| Months 6 to 12 | Weeks 25 to 52 | Full recovery for 80 to 90% of patients. Fascia tissue is structurally remodeled. |
| Beyond 12 months | Year 2+ | Chronic cases (10 to 20% of patients). Time to consider ESWT, PRP, or surgical evaluation. |
The single biggest mistake patients make: stopping the stretches and supportive shoes once symptoms improve. The fascia takes longer to fully remodel than the symptoms take to fade. Continue the routine for at least a month past symptom resolution.
When to see a clinician
- Heel pain that hasn’t improved after 4 to 6 weeks of consistent stretching and supportive shoes
- Pain at night or at rest (suggests other causes)
- Inability to walk normally
- Swelling, warmth, or visible redness at the heel
- A specific moment of injury or a “pop”
- You have diabetes or peripheral neuropathy — any heel pain deserves evaluation
- Recurrence after previous successful treatment
- A child with heel pain (consider Sever’s disease)
Prevention
Once you’ve had plantar fasciitis, you’re more likely to get it again. Reduce recurrence with:
- Daily calf and foot stretches, even after symptoms resolve
- Replace running shoes every 300 to 500 miles
- Build mileage gradually (the 10% rule is a starting point, not a guarantee)
- Avoid going barefoot on hard floors at home
- Maintain a healthy weight
- Address tight calves as an ongoing priority, not just during a flare
- Rotate shoes so each pair has 24+ hours to dry and decompress
- Stretch before getting out of bed in the morning: ankle circles, towel pulls, gentle toe pulls. The first step pain is dramatically reduced if the fascia is gently woken up first.
Bottom line
Plantar fasciitis is the most common cause of heel pain, and roughly 80 to 90% of cases resolve within 6 to 12 months with consistent conservative care: stretching twice daily, supportive shoes worn all day, and patience. The single most underrated driver is tight calf muscles (equinus), and the single most underrated treatment is the plantar fascia-specific stretch (toes pulled back toward the shin). The two most overrated approaches are repeat cortisone injections and buying expensive insoles without addressing the calves. Surgery is rarely needed and reserved for cases that have failed a year or more of conservative care.
If your pain doesn’t fit the classic morning-stabbing pattern, or it isn’t responding after 4 to 6 weeks, see a clinician — several other conditions can mimic plantar fasciitis and respond to different treatment.
Frequently asked questions
How long does plantar fasciitis last?
Most cases resolve within 6 to 12 months — that's the natural history. About 80 to 90% of patients recover without surgery. Active treatment (custom orthotics, daily stretching, physical therapy) often accelerates this significantly: many patients see meaningful relief within 6 to 12 weeks when they commit to the routine. Cases ignored or pushed through tend to last longer than cases addressed early.
Can plantar fasciitis go away on its own?
Sometimes yes. About 80% of cases resolve within a year even with minimal treatment. But ignoring it usually means a longer, more painful course and a higher chance of compensating gait that triggers other foot or knee problems. Early stretching, ice, and footwear changes shorten healing time significantly.
Why does plantar fasciitis hurt more in the morning?
Overnight, the plantar fascia tightens while the foot rests in plantarflexion (toes pointed). The first morning steps suddenly stretch that tightened tissue, causing the classic stabbing heel pain. Pain typically eases after a few minutes of walking as the fascia warms up and lengthens, then returns after long sitting or at the end of the day.
Should I walk with plantar fasciitis?
Walking is generally OK and can actually help by preventing the fascia from stiffening. The key changes: avoid being barefoot on hard floors, don't push through sharp pain, and wear supportive shoes (even at home). Shorter walks are better than long sessions on hard surfaces. Reduce running temporarily; cross-train with cycling or swimming if you need cardio.
What is the fastest way to relieve plantar fasciitis?
There's no instant fix, but consistent relief often comes from a combination of: (1) supportive shoes or orthotics worn all day including at home, (2) calf and plantar fascia stretching morning and evening, (3) ice rolling the arch for 10 to 15 minutes after activity, and (4) avoiding barefoot walking. Most people feel meaningful improvement within 2 to 4 weeks of consistent care.
When should I see a doctor for plantar fasciitis?
See a clinician if pain hasn't improved after 4 to 6 weeks of conservative care, if pain is severe enough to limit walking, if there's pain at night or at rest, or if you have diabetes or neuropathy. A podiatrist can confirm the diagnosis (other conditions can mimic plantar fasciitis), prescribe stronger treatment, or rule out more serious problems like a calcaneal stress fracture or tarsal tunnel syndrome.
What's the single best stretch for plantar fasciitis?
The most evidence-supported stretch is the **plantar fascia-specific stretch**: sit down, cross the affected foot over the opposite knee, grasp the toes, and pull them back toward the shin until you feel a stretch in the arch. Hold 10 seconds, repeat 10 times, three times daily. A 2003 randomized trial showed this stretch outperforms standard calf stretching for plantar fasciitis. Calf stretching helps too (especially gastrocnemius stretches against a wall), but the toe-back stretch directly targets the fascia.
Are night splints worth it for plantar fasciitis?
For stubborn cases (lasting more than a few months), yes. Night splints hold the foot at 90 degrees so the fascia doesn't tighten overnight, which directly addresses the morning pain mechanism. They're awkward to sleep in for the first few nights, and many patients abandon them too soon. For people willing to wear them consistently for 4 to 6 weeks, the morning pain reduction is often dramatic. Sock-style splints (like the Strassburg Sock) are usually better tolerated than rigid boot-style splints.
Should I get a cortisone shot for plantar fasciitis?
Cortisone injections offer real short-term relief (weeks to a few months), but they have a downside: repeated injections can weaken the plantar fascia, thin the heel fat pad, and increase the risk of fascial rupture. Practice on frequency varies: a cautious protocol limits cortisone to one or two injections per heel per lifetime; more common practice allows up to 3 per year for stubborn cases. Either way, each injection carries cumulative risk. Newer alternatives like platelet-rich plasma (PRP) and shockwave therapy (ESWT) are increasingly preferred for chronic cases because they don't carry the rupture risk.
What's the difference between plantar fasciitis and a heel spur?
Heel spurs are bony growths on the underside of the heel bone, often discovered incidentally on X-ray. Plantar fasciitis is the soft-tissue irritation of the fascia. The two are commonly found together, but **the spur itself is rarely the source of pain** — surrounding soft tissue (most commonly the plantar fascia) is. Many people have heel spurs visible on X-ray with no pain at all. Treatment focuses on the fascia, not the spur.
Will losing weight help plantar fasciitis?
If you're carrying extra weight, yes. Every step puts force several times your body weight through the heel and arch. Studies show that body mass index correlates strongly with plantar fasciitis incidence and severity. Even a modest 5 to 10% weight reduction often translates to noticeable symptom improvement, though this approach is a slower lever than stretching and shoe changes.
Sources
Last updated: May 4, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 4, 2026