
What they are
Accessory ossicles are extra small bones present in the foot from birth. They form when an additional center of bone formation (an “ossification center”) doesn’t fuse with the main bone next to it during development — leaving a small separate ossicle that persists for life.
They are normal anatomical variants, not abnormalities or fractures. But because they look similar to fractures on X-ray, distinguishing them matters clinically.
How common are they?
Roughly 1 in 5 adults has at least one accessory ossicle in the foot. Some are very common — bipartite sesamoids appear in 10–30% of people; the accessory navicular in 4–14%; the os trigonum in about 7–10%. Others are rare.
Most are discovered incidentally — on X-rays taken for unrelated reasons — and never cause symptoms.
Common types and locations
Several accessory ossicles are well-recognized clinically. The most relevant ones for foot health:
- Accessory navicular (also called “os tibiale externum”) — extra bone on the medial midfoot, next to the navicular. The most common symptomatic accessory ossicle. Often pulls on the posterior tibial tendon and causes arch pain.
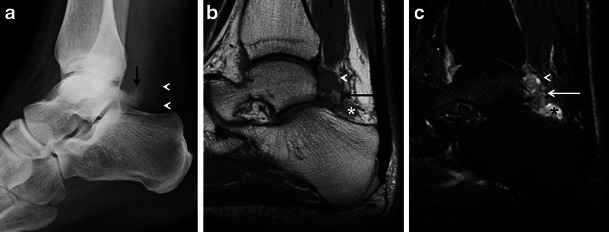
- Os trigonum — extra bone behind the talus at the back of the ankle. Can get pinched with hyperplantarflexion (ballet, soccer kicks) — see posterior ankle impingement.
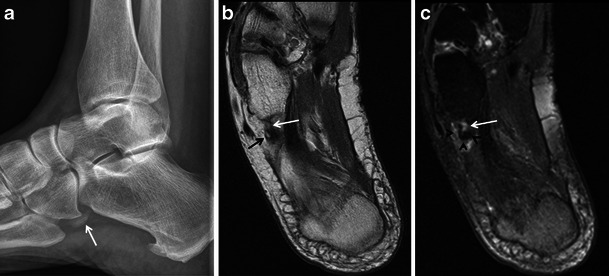
- Os peroneum — embedded within the peroneus longus tendon along the lateral foot. Can fracture or contribute to lateral foot pain (“painful os peroneum syndrome”).
- Os intermetatarseum — between the bases of the 1st and 2nd metatarsals on the top of the foot. Usually silent.
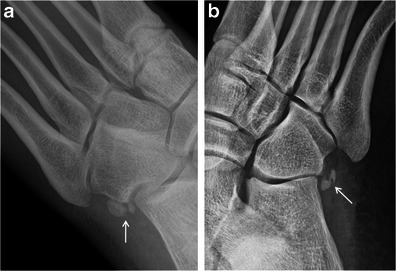
- Os vesalianum — at the lateral base of the 5th metatarsal. Can be mistaken for a Jones fracture on X-ray.
- Bipartite sesamoid — one of the sesamoid bones under the big toe joint formed in two pieces instead of one. Easily confused with a sesamoid fracture.
Many others exist (os subtibiale, os subfibulare, os supratalare, os calcaneus secundarius, etc.), but symptomatic cases of those are uncommon.
Examples on imaging
When they cause problems
Most accessory ossicles never become symptomatic. When they do, it’s usually one of these patterns:
- Direct pressure or impingement — the ossicle gets pinched between adjacent bones during certain movements (os trigonum is the classic example, with pointing the foot down)
- Irritation of an attached tendon — the accessory navicular pulls on the posterior tibial tendon; the os peroneum sits within the peroneus longus tendon
- Fracture or separation of the ossicle — uncommon, but happens after acute injury or with stress
- Bony prominence — a few accessory ossicles cause a visible or palpable bump that rubs against shoes
- Mistaken for a fracture — on X-ray, a normal accessory ossicle can look like a broken fragment, and vice versa. Sorting this out is one of the most common reasons to image these areas in the first place.
How they’re diagnosed
- X-ray — most accessory ossicles are visible on plain films. Smooth, well-corticated edges suggest a true accessory ossicle; irregular or jagged edges suggest a fracture.
- MRI — useful when an accessory ossicle is symptomatic, to look for surrounding inflammation or stress reaction in the bone
- CT — sometimes used when fracture vs. accessory ossicle remains unclear after X-ray
- Bone scan — can show increased uptake at a symptomatic accessory ossicle, supporting that it (rather than something incidental) is the source of pain
Comparison to the opposite foot helps — accessory ossicles are often bilateral, while fractures usually aren’t.
Treatment
Asymptomatic accessory ossicles need no treatment.
For symptomatic cases, treatment depends on the specific ossicle:
- Activity modification, ice, and NSAIDs for inflammation flares
- Padding or shoe modification to relieve pressure on prominent ossicles
- Custom orthotics when the ossicle affects foot mechanics (common with the accessory navicular)
- Walking boot or cast for stress reactions or stubborn cases
- Cortisone injection for chronic inflammation around an accessory ossicle
- Surgical excision — reserved for ossicles that fail prolonged conservative care and are clearly the source of symptoms
Bottom line
Accessory ossicles are common normal variants — most go through life undetected. When pain develops in a typical foot location, an X-ray showing an accessory ossicle is helpful but not always definitive: many people have asymptomatic accessory ossicles AND a different cause for their pain. An in-person evaluation by a clinician — sometimes with additional imaging — determines whether the ossicle is actually the source of symptoms or just an incidental finding.
Sources
Last updated: May 3, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: May 3, 2026