What it is
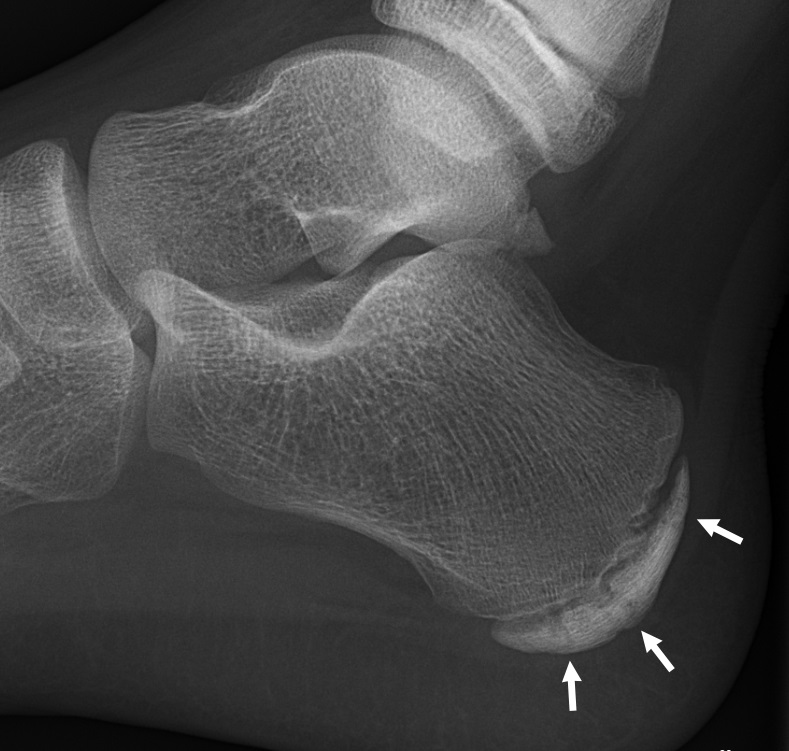
Despite its name, Sever’s disease isn’t really a disease — it’s an overuse injury to the growth plate (apophysis) at the back of the heel bone. The growth plate is a band of cartilage at the bottom of the calcaneus where the bone is still actively growing. The Achilles tendon attaches just above it.
During the growth spurt years (roughly 8–14), the heel bone grows faster than the surrounding muscles and tendons can keep up. The Achilles tendon gets pulled tight. Repeated impact from running and sports irritates the growth plate at the heel attachment, producing inflammation and pain.
Two important things to know:
- It’s self-limiting. Symptoms typically resolve completely once the growth plate fuses, usually by age 14–16.
- It doesn’t cause permanent damage. Long-term outcomes are excellent.
Symptoms
The classic presentation is an active child or young teenager with:
- Pain at the back or bottom of one or both heels — often worse on one side
- Pain that’s worse during and after sports, especially running, jumping, and cleated shoes
- Limping after activity, sometimes with reluctance to walk on the heel (toe-walking)
- Tenderness when the sides of the heel are squeezed (the “squeeze test”)
- Stiffness in the morning that loosens up with movement
- Symptoms that improve with rest
Pain is typically bilateral in about 60% of cases, although one side is usually more affected.
What causes it
Sever’s is fundamentally an imbalance: heel bone growing fast, soft tissues lagging behind, repetitive impact loading.
Common contributors:
- Recent growth spurt — the immediate trigger in many cases
- Sport season ramping up — especially soccer, basketball, gymnastics, track
- Tight calf muscles
- Hard surfaces (asphalt, wood gym floors)
- Worn-out shoes with limited heel cushioning
- Cleats — the rigid heel cup pushes directly into the growth plate
- Foot mechanics — flat feet or high arches can predispose
Diagnosis
Sever’s is a clinical diagnosis — the history (active child, age 8–14, growth spurt, heel pain after sports) and physical exam (tenderness with the squeeze test) are usually all that’s needed. X-rays are typically not necessary.
X-rays may be done if:
- The pain is severe or limiting walking
- There’s significant swelling, redness, or warmth
- The pain is unilateral and persistent (to rule out a stress fracture or other cause)
- Symptoms haven’t improved after several weeks of treatment
Treatment
The good news: this responds very well to conservative care. The aim is to reduce stress on the growth plate while it’s still vulnerable.
Activity adjustment
- Reduce — don’t necessarily stop — sports during a flare-up. A 1–2 week break from the offending activity often helps significantly.
- Cross-train with low-impact options: swimming, cycling, elliptical
- Resume gradually as pain improves
Footwear and padding
- Heel cups or gel pads placed in shoes — often dramatically helpful
- Supportive, cushioned athletic shoes (replace old or worn ones)
- Avoid going barefoot on hard surfaces at home during flares
- Avoid cleats when possible, or add a heel pad inside
Stretching and strengthening
- Calf stretches several times daily — both straight-knee (gastrocnemius) and bent-knee (soleus) stretches
- Plantar fascia stretches — pulling toes back gently
- Toe-to-knee ankle range-of-motion exercises
- These help prevent recurrence, not just the current episode
Symptom management
- Ice after activity for 15–20 minutes
- NSAIDs (ibuprofen, naproxen) for pain — used short-term
- Over-the-counter heel cushions
When more is needed
If the above isn’t enough after a few weeks:
- A short course in a walking boot to fully offload the heel (1–3 weeks)
- Physical therapy for a tailored stretching/strengthening program
- Rarely, a brief period of casting for severe cases
Steroid injections are not recommended for Sever’s disease — they can weaken the growth plate.
When to see a clinician
Get evaluated if:
- Pain persists more than 2–3 weeks despite rest and heel cups
- The child can’t bear weight or is severely limping
- There’s significant swelling, redness, warmth, or fever
- Pain is one-sided and severe (to rule out stress fracture)
- The child is outside the typical age range (younger than 7 or older than 14) — other causes become more likely
Prevention
Once the current episode resolves, simple habits reduce the risk of future flares:
- Daily calf stretching, especially in the months leading up to a sports season
- Replace athletic shoes every 6 months for active kids (or sooner if visibly worn)
- Use heel pads preventively in cleats and stiff shoes
- Build into new sports gradually — avoid sudden ramps in mileage or practice intensity
- Listen to early warning signs — a few days of rest at the first twinge often prevents a multi-week flare
Living with it
Most kids return to full sports within a few weeks. The condition often returns during another growth spurt or new sport season but is rarely as severe the second time. By age 14–16, when the growth plate fuses, Sever’s disappears for good.
Reassure the child: this is real pain, but it’s temporary, and it doesn’t mean anything is seriously wrong with their foot. Some kids worry they have a “broken bone” or a serious injury — knowing it’s a normal part of growing helps them stay engaged in activity within the modified plan.
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026