Quick answer
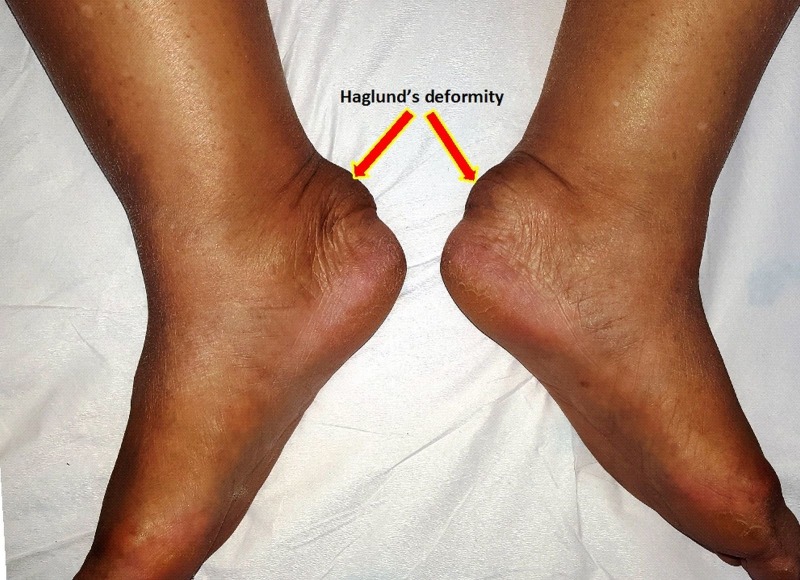
Haglund’s deformity is a bony prominence at the back of the heel bone (calcaneus). The bump itself doesn’t hurt — what hurts is the soft tissue around it: an inflamed bursa and sometimes the Achilles tendon attachment. The “pump bump” nickname comes from the classic association with stiff-backed pumps that rub on the prominence.
How to recognize it
- Visible bump at the back of the heel, sometimes red or thickened skin over it
- Pain at the back of the heel with stiff-backed shoes
- Tenderness when pressed at the bump
- Worse with high heels, dress shoes, ice skates, ski boots, cleats
- Better in soft-backed or open-backed shoes
- Sometimes coexists with insertional Achilles tendinitis — pain right where the Achilles attaches
What’s actually happening
Three things are typically going on:
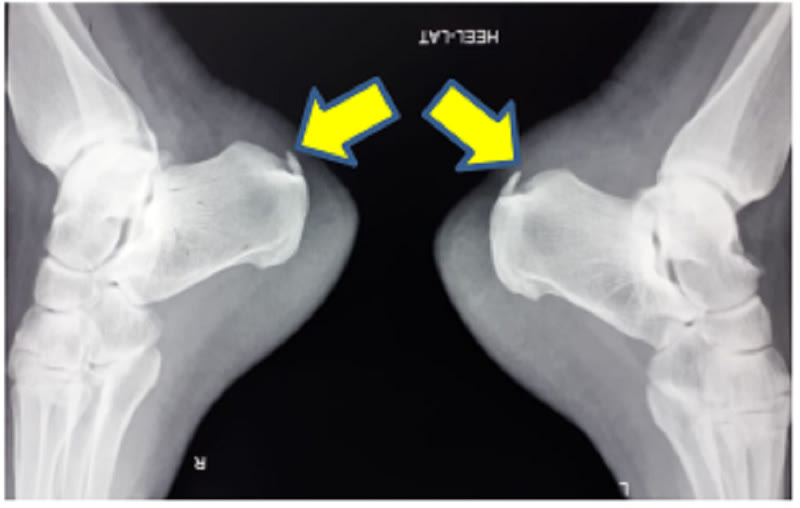
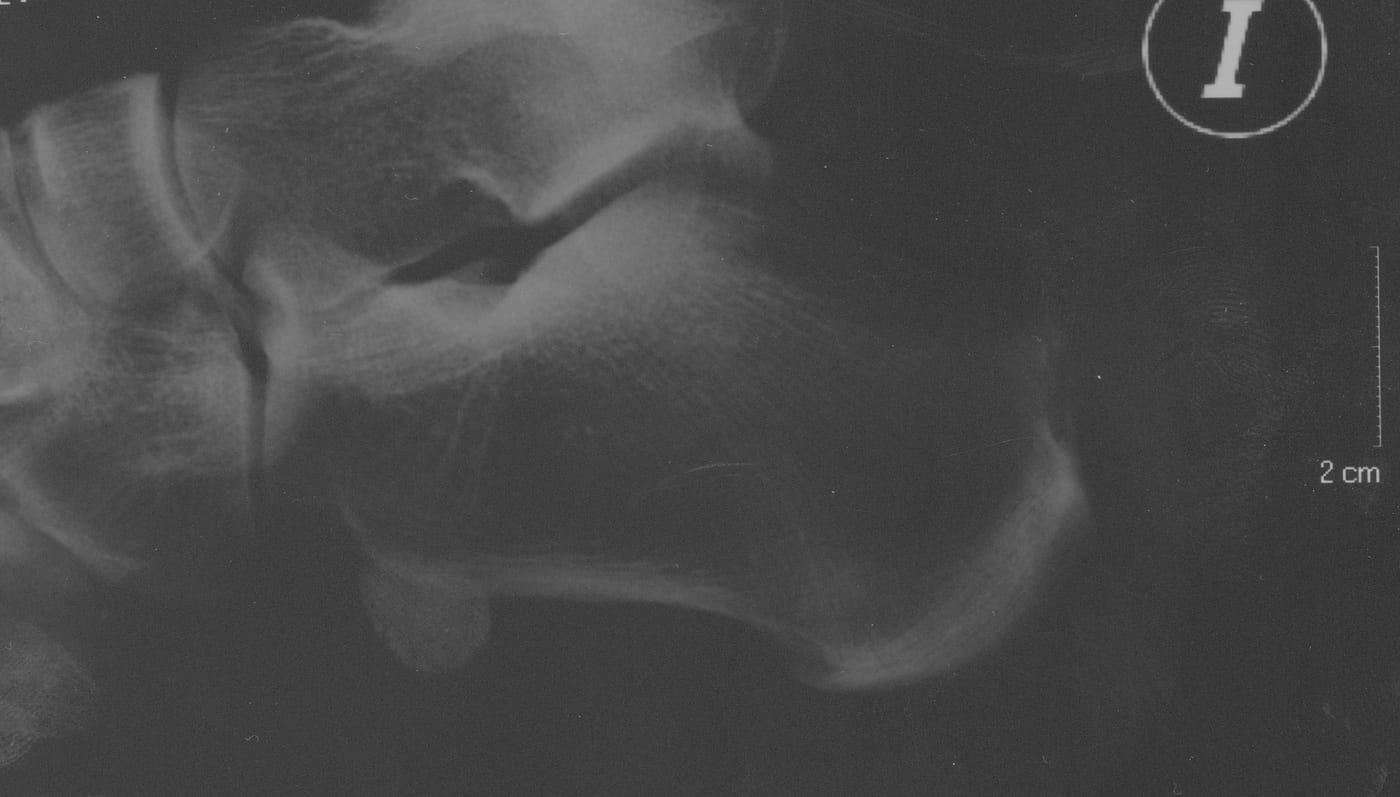
- The bony bump — a prominence at the upper-outer back of the heel bone. Often a normal anatomical variant some people are born with.
- Retrocalcaneal bursitis — inflammation of the bursa between the heel bone and the Achilles tendon
- Achilles tendinopathy — irritation where the tendon attaches to the heel
The combination is sometimes called the “Haglund’s syndrome.” Not everyone with the bony bump has pain — symptoms appear when shoe pressure or activity inflames the surrounding tissues.
Why it happens
- Stiff shoe heel counters — pumps, dress shoes, work boots, ice skates, ski boots, cleats all have rigid heel cups that press on the bump
- Repetitive impact — running, especially uphill or in worn shoes
- High arches (cavus foot) — tend to angle the heel, putting more contact on the bump
- Tight Achilles / calf — increases tension at the heel attachment
- Inherited foot shape — the bony anatomy is largely genetic
What to do about it
Conservative care (resolves most cases)
- Change footwear — open-back shoes, soft-back shoes, mules — anything that doesn’t press on the bump
- Heel pads or lifts — raise the heel slightly so the bump sits above the shoe’s heel counter
- Soft padding over the bump (silicone gel sleeves)
- Stretching — calf and Achilles
- NSAIDs for short-term pain
- Ice after activity
- Reduce aggravating activities — running, hill walking
- Custom orthotics with a heel lift for high-arched feet
When initial measures aren’t enough
- Physical therapy — eccentric Achilles loading, calf strengthening
- Walking boot for 2–4 weeks for severe flares
- Steroid injection — used cautiously due to risk of Achilles tendon weakening; never injected directly into the tendon
- Extracorporeal shock wave therapy (ESWT) — option for chronic cases
Surgery (last resort)
For cases that fail 6–12 months of conservative care:
- Bony resection (Haglund’s procedure) — removing the prominence
- Achilles debridement if degenerative changes are present
- FHL tendon transfer for severe Achilles damage
Recovery is significant — typically 6–12 weeks in a boot, gradual return to activity, full recovery often 6+ months.
When to see a clinician
- Pain limiting your shoe choice or activities
- Visible skin breakdown over the bump
- Pain that’s worsened despite shoe changes
- Recurrent flare-ups
- Pain at the back of the heel that’s spreading or getting worse over time
- You have diabetes — closer attention to skin changes is important
Prevention
- Avoid stiff-backed shoes for prolonged daily wear
- Choose shoes with soft, padded heel counters
- Heel pads in shoes that put pressure on the bump
- Stretch calves daily
- Replace worn shoes
- Address tight calves with a stretching routine before they cause issues
Last updated: April 25, 2026

About the author
Written and reviewed by a Doctor of Podiatric Medicine (DPM) practicing in Arizona for 6+ years. Board-certified by the American Board of Podiatric Medicine (ABPM); graduate of Midwestern University Arizona College of Podiatric Medicine.
Last clinically reviewed: April 25, 2026